Article Text

Abstract
A man in his 50s presented to the eye emergency department on three separate occasions complaining of blurred vision and discomfort in the left eye. He had a history of Marfan syndrome and had undergone bilateral 20-gauge (G) pars plana vitrectomy and lensectomy 20 years prior for ectopia lentis. On examination he had epithelial corneal oedema, raised intraocular pressure >40 mm Hg and conjunctival chemosis, which later appeared as a bleb-like conjunctival elevation. Acute treatment with oral acetazolamide and topical ocular hypotensive agents produced a marked reduction in intraocular pressure to 2–4 mm Hg. A presumed diagnosis of a leaking scleral wound was made. He underwent scleral exploration under general anaesthesia and a leaking sclerotomy was uncovered. The defect was repaired successfully using a scleral patch graft. Late dehiscence of a sclerotomy has been reported rarely in patients with Marfan syndrome. This is the first reported case to present atypically with intermittent episodes of raised intraocular pressure rather than with hypotony.
- Ophthalmology
- Connective tissue disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Marfan syndrome is an autosomal dominant connective tissue disorder caused by a mutation in the fibrillin-1 gene that affects the eyes, skeletal and cardiovascular systems.1 The most common ocular feature of Marfan syndrome is bilateral ectopia lentis, which is displacement of the lens from its normal position.2 Subluxation of the lens is most frequently superotemporal in Marfan syndrome.3 Other common ocular manifestations of Marfan syndrome include axial myopia, lattice degeneration and consequent retinal tears or detachment, iris hypoplasia and strabismus.3 Rare cases of spontaneous scleral perforation have been reported.4 5
Ectopia lentis can be managed conservatively with refractive correction or surgically with lens extraction with or without intraocular lens implantation.3 Depending on the degree of dislocation, a posterior approach with vitrectomy and lensectomy may be required. Reported complications of vitrectomy in Marfan patients include retinal detachment, transient ocular hypertension or lens implant-related complications.6 Prior cases of sclerotomy dehiscence post vitrectomy in patients with Marfan syndrome have been described.7 8 These cases presented as a hypotonus eye with Seidel positivity at a previous sclerotomy. We report a case of late-onset sclerotomy dehiscence presenting with intermittent episodes of raised intraocular pressure.
Case presentation
A man in his 50s presented to the eye emergency department complaining of blurred vision and mild discomfort in the left eye, which he noticed after putting in his contact lenses. He had a background history of Marfan syndrome and had undergone bilateral 20G pars plana vitrectomy and lensectomy for ectopia lentis 20 years prior. He wore rigid contact lenses to correct for aphakia. On examination, the best corrected visual acuity in the left eye was 0.5 LogMAR, compared with 0.3 LogMAR in the right eye. Slit lamp examination of the left eye revealed epithelial corneal oedema, conjunctival chemosis and raised intraocular pressure at 42 mm Hg. There was no anterior chamber inflammation and the angle was wide open on gonioscopy (grade 4 Shaffer), with no angle recession, normal pigmentation and no angle neovascularisation. There was no ultrasound biomicroscopy available to further explore the angle anatomy. The cup to disc ratio was 0.4 in both eyes. There was no history of eye injury.
The patient was treated with oral Diamox (acetazolamide) 500 mg stat (2 tablets of 250 mg together) followed by 250 mg four times a day in addition to maximum topical intraocular pressure lowering treatment with Duotrav (travoprost and timolol) 1 drop at night and Simbrinza (brinzolamide and brimonidine tartrate) 1 drop every 12 hours. This produced a dramatic reduction in intraocular pressure to 2–4 mm Hg within 24 hours. At this stage, the acetazolamide was stopped. All topical ocular hypotensive agents were subsequently discontinued within 4 weeks. Remarkably, the patient’s intraocular pressure remained very low for weeks after stopping all treatment. Despite having a hypotonus eye, the patient’s vision fortunately, recovered fully being asymtpomatic. He did not develop maculopathy secondary to hypotony. The optical coherence tomography (OCT) of optic disc and macula and Humphrey visual field test 24–2 SITA (Swedish Interactive Threshold Algorithm) standard were normal in both eyes.
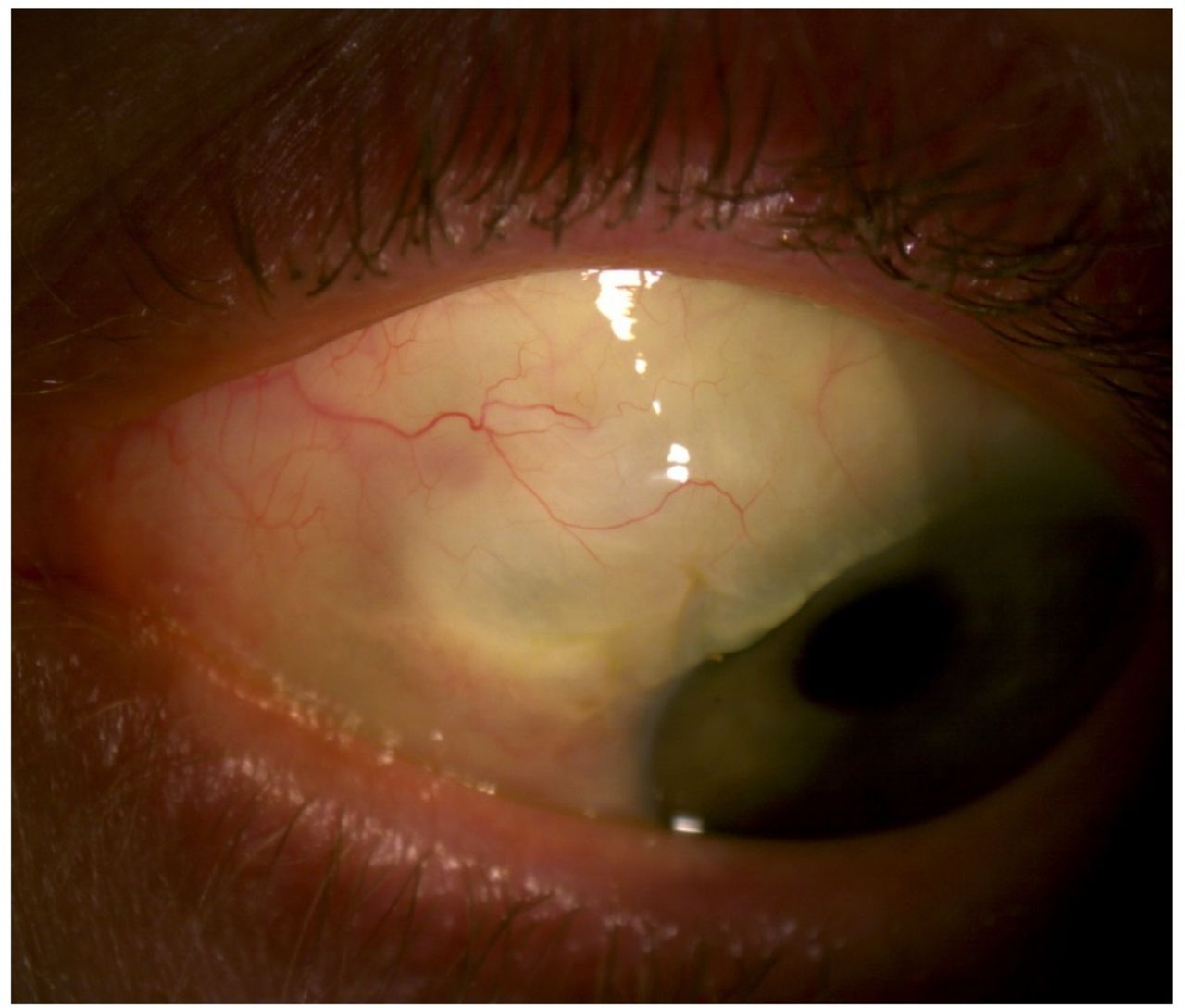
Due to the COVID-19 pandemic, the patient was not reviewed as planned in the outpatient department. However, he represented on a further two occasions to the eye emergency department with recurrence of symptoms, corneal oedema and a raised intraocular pressure of 43 and 45 mm Hg. On these presentations, it was noted that there was a bleb-like conjunctival elevation superonasal to the limbus (figure 1). Intraocular pressure lowering therapy identical to the first episode was initiated on each presentation but stopped after a few weeks due to hypotony. A presumed diagnosis of a late onset sclerotomy dehiscence post 20G vitrectomy was made. This diagnosis accounted for the conjunctival bleb and marked hypotony in response to intraocular pressure lowering agents, however, the explanation of the episodes of raised pressure remains challenging. The highly plausible mechanism for the episodes of raised intraocular pressure was that the sclerotomy was leaking chronically leading to increased aqueous humour production as a feedback mechanism. Transient closure of the sclerotomy with granulation tissue resulted in the intraocular pressure spikes. Prior to these three acute presentations, the patient was followed only by his optician on a 2 yearly basis having had recorded intraocular pressures within the normal range.

Preoperative photograph of patient’s left eye showing superonasal conjunctival bleb.
Treatment
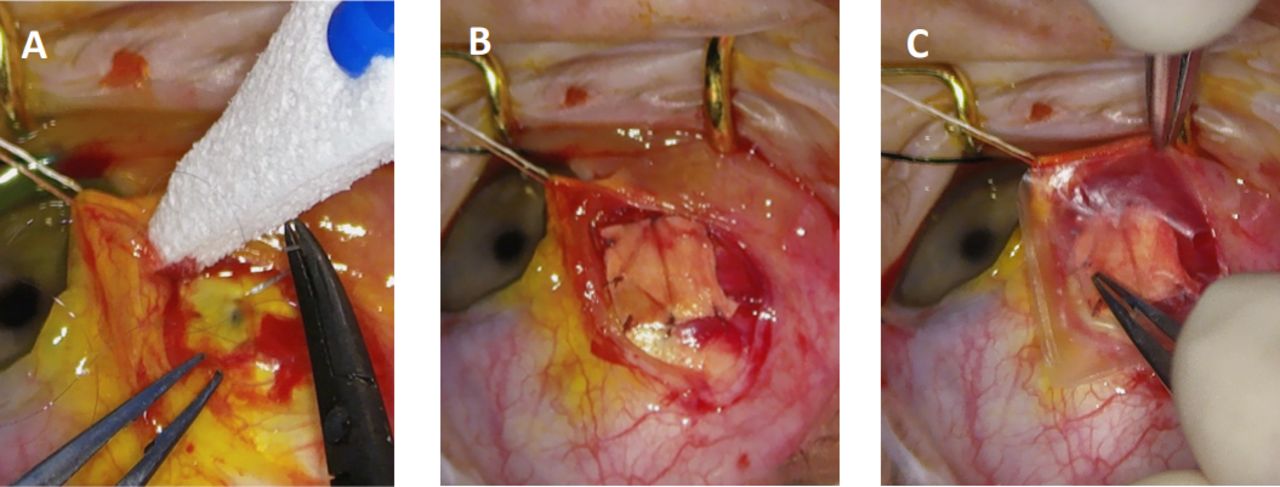
Wound exploration was carried out under general anaesthesia. A conjunctival peritomy allowed examination of the sclera. A small scleral wound was identified 4 mm from the limbus in the superonasal quadrant (figure 2A). Fluorescein 2% application confirmed leakage from the wound. The wound was directly closed with 10–0 vicryl. Additionally, a scleral patch graft was sutured over the wound with 8–0 vicryl (figure 2B), and further sealed with fibrin glue. An Omnigen dried amniotic membrane was placed over the scleral patch graft to protect the thin overlying conjunctiva (figure 2C), which was closed with 8–0 vicryl. Subconjunctival ceftazidime and dexamethasone were administered at the end of the procedure.

Intraoperative photographs: (A) Identification of the leaking sclerotomy. Fluorescein application demonstrated Seidel positivity. (B) Scleral patch graft in situ. (C) Amniotic membrane placement over scleral graft.
Outcome and follow-up
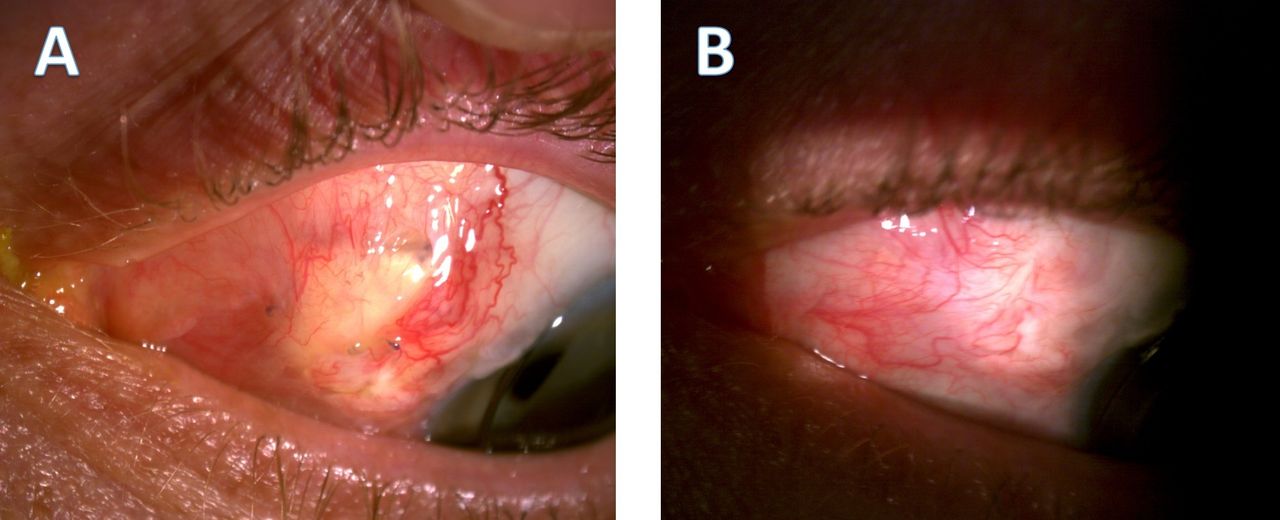
Our patient obtained a very good outcome at 9 months follow-up, with visual acuity stabilising at 0.3 LogMAR. Figure 3A shows the scleral graft with overlying conjunctiva at 1 month postoperatively. Figure 3B shows the graft at 9 months postoperatively with a resolution of subconjunctival fluid. Intraocular pressure has remained at 16 mm Hg postoperatively without the use of any intraocular pressure lowering agents. He had no evidence of glaucomatous visual field loss on Humphrey field testing, and his OCT of the optic disc remained normal.

{kind=link}
{kind=link}
{kind=link}
Postoperative photographs of the left eye showing healed conjunctiva overlying scleral patch graft at (A) 1 month postoperatively and (B) 9 months postoperatively.
Discussion
We report an atypical presentation of a late sclerotomy wound dehiscence in a patient with Marfan syndrome. Abnormal fibrillin-1 results in a thin sclera in Marfan patients. A number of cases of spontaneous scleral rupture have been published.5 9 There have also been reports of erosion of the scleral buckle leading to hypotony in Marfan syndrome.10 11 Sclerotomy dehiscence has been previously described after vitrectomy-lensectomy.7 8 All of the above patients presented with low intraocular pressure, as would usually be expected with an open globe.
The clinical picture in this case was atypical because the patient had an open globe, but at acute presentations to the eye emergency department, the intraocular pressure was very high. There are a few possible explanations for this. First, it is possible that the sclerotomy was leaking chronically leading to increased aqueous humour production as a feedback mechanism, and transient closure of the sclerotomy resulted in the intraocular pressure spikes. Treatment with acetazolamide and topical ocular hypotensives produced an exaggerated reduction in intraocular pressure, likely due to the reopening of the sclerotomy. Alternatively, it is also possible that raised intraocular pressure had in fact led to the dehiscence of the scleral wound. Since surgical repair of the scleral leak; however, our patient has had no further episodes of raised intraocular pressure, making the latter scenario less plausible.
Traditionally, vitrectomy was carried out through 20G ports, with instrumentation having a relatively wide diameter of 0.9 mm.12 This has largely been replaced by smaller 23G techniques, or even sutureless 25G and 27G systems.12 A leaking sclerotomy post vitrectomy is usually managed by suturing the wound closed. In the case of a thin sclera such as that in Marfan syndrome, closure of the scleral defect with a scleral patch graft is more appropriate. Scleral patch grafts are most frequently used in the management of scleral thinning due to necrotising scleritis.13 A similar technique was used in other cases of scleral defects in Marfan syndrome.4 8 With the decline of 20G vitrectomy we can hope to see even fewer of these rare cases.
Learning points
Sclerotomy dehiscence is a rare potential complication in patients with connective tissue disease that can occur late after vitrectomy such as in this patient with Marfan syndrome.
Sclerotomy dehiscence may present atypically with acute raised intraocular pressure against a background of chronic hypotony.
Scleral patch grafting is an effective management option for the repair of scleral defects in Marfan syndrome.
Patients with Marfan syndrome should not be discharged from the eye clinic. They should instead be kept in regular review for related ocular complications. Patients should be informed about the possible complications.
Ethics statements
Patient consent for publication
Footnotes
Twitter @PaulEStanciu
Contributors PES: acquisition of data, conception and design, analysis and interpretation of data, management of case. AO: conception and design, analysis and interpretation of data. EC: diagnosis and management of case, revision of article for important intellectual content and final approval of the version published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.