Article Text

Abstract
We present a rare complication of microwave ablation (MWA) in a male patient in his 80s. His massive pulmonary necrosis and tension pneumothorax required urgent surgery. However, the damage to the lung tissue was too large, deep and fragile. We failed to suture or conduct wedge resection on the lung lesion, so, left upper lobectomy was necessary. Therefore, we suggest that it is probably possible to reduce the frequency and time threshold when performing MWA for the elderly with comorbidities.
- Cancer intervention
- Lung cancer (oncology)
- Radiotherapy
- Pneumothorax
- Cardiothoracic surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Indications for thermal ablation therapy in lung cancer include: primary non-small-cell lung cancer (NSCLC) with contraindications for surgery and focal lung metastatic lesions that originate from multiple other tumour types, including colorectal cancer, sarcoma, kidney, hepatocellular carcinoma, breast and neuroendocrine tumours.1 In addition, a review study showed that 0.4% of patients with cancer had indications but refused surgery due to the following risk factors: advancing age, decreasing annual income, non-white race and unmarried status.2 We present a rare complication of microwave ablation (MWA) in an old male with NSCLC (T1cNoMo) who refused surgery. After ablation, the patient developed massive pulmonary necrosis and tension pneumothorax. Surgical repair was successfully performed using urgent video-assisted thoracic surgery (VATS) pulmonary lobectomy.
Case presentation
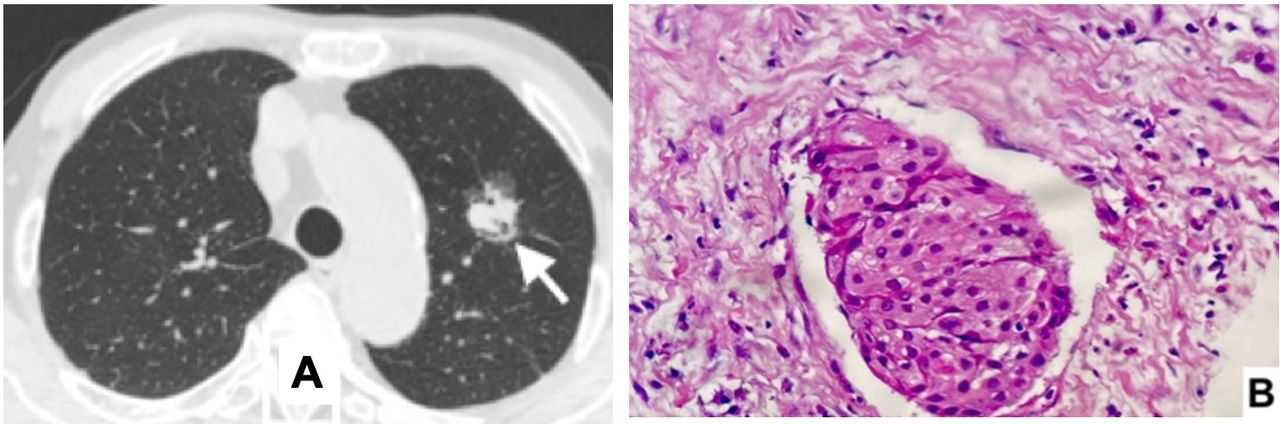
A male patient in his 80s with a 4-month history of lung nodules was admitted to our hospital for further investigation of the lung lesions. The CT of lung lesions at that admission was shown in figure 1A. He has had hypertension for 10 years, treated with an ACE inhibitor; right colic cancer with curative surgery for 2 years and prostate hypertrophy with embolisation for 1 year.

Lung lesion in CT and biopsy before MWA. (A) 2.0 cm in diameter lung nodule in the upper left lobe 4 months before admission. (B) Squamous cell carcinoma with lymphatic invasion
Investigations
During this hospitalisation, chest CT revealed a 2.8 cm nodule in the left upper lobe without a notable mediastinal lymph node and his whole-body MRI demonstrated non-extra lung lesion (T1cNoMo). CT-guided percutaneous lung biopsy of the lesion confirmed as squamous cell carcinoma (T1cNoMo) (figure 1B). The pulmonary function test was normal.
Treatment
The patient and his family were consulted with the indication of VATS left upper pulmonary lobectomy and mediastinal lymph node resection. The patient refused surgery while considering his age, higher than the expected longevity of local male elders, associated with previous colon cancer treatment, and the patient’s personal point of view that surgery for lung cancer may be ineffective and accelerate the overall deterioration of these cancers. He underwent MWA under CT guidance, and 2 min ablation with 915 Hz microwave frequency was used. The immediate result was uneventful (figure 2).

Application of MWA. (A) CT-guided puncture. (B) Application of ablation. (C) Early result of MWA. MWA, microwave ablation.
Outcome and follow-up
The patient was stable for 3 days. On the fourth day, he developed progressive shortness of breath. Chest CT showed pneumothorax. Two chest tubes were placed in the second and sixth intercostal space to reduce symptoms (figure 3A).

Complication and lesion after MWA. (A) Left pneumothorax. (B) The removed upper left lobe with massive necrotic lesion. MWA, microwave ablation.
After chest placement, subcutaneous emphysema progressed rapidly to the neck and face and the respiratory symptoms did not relieved. Urgent surgery was done on the fourth day after MWA. Lung lobectomy had to be performed due to difficulty in controlling the bleeding and air leakage at the inflammatory area of massive thermal lung tissue (figure 3B). The pathological results of the specimen were squamous cell carcinoma, hyaline degeneration, necrosis of normal lung and tumour tissue (figure 4). The patient recovered after 5 days in intensive care unit and was discharged 20 days after surgery.
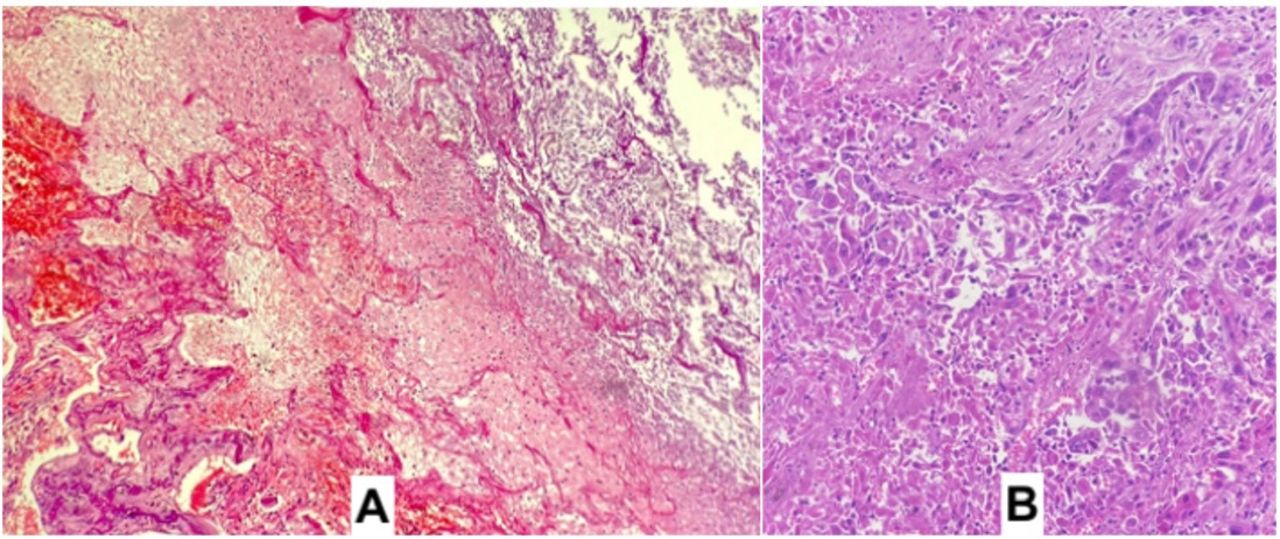
Microscopic image of necrotic lung. (A) Hyaline degeneration and necrosis of normal lung and tumour tissue. (B) The remaining cancer cells among hyaline degeneration areas.
He was reexamined after discharge at 1, 6 and 9 months without any notable problems. The 12th month examination was postponed due to COVID-19 pandemic. More than 1 year later, he developed haemoptysis, and CT showed metastatic tumours in the right lung and mediastinum with invasion (figure 5). After consultation, the patient refused any further treatment. He died nearly a year and a half after the surgery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Recurrent metastatic progression. (A) Contralateral lung metastasis. (B) Recurrent tumour with bronchial and pulmonary arterial invasion.
Discussion
Surgical resection is the curative therapeutic option of choice in early-stage NSCLC, but other treatments could be considered if the patients refuse it. Among thermal ablation therapies, MWA has shown less heatsink effect than radiofrequency ablation in the treatment of hepatic cancer.3 Similar results were observed in lung lessions.4 The main advantages of microwave technology, when compared with existing thermal ablation therapies, include higher intratumoural temperatures, larger treatment volumes, faster treatment times and an improved convection profile,5 which were the reasons for this as the treatment of choice in this case.
The most commonly reported complications of MWA is pneumothorax, with rates of 8,5%–63% and 0.8%–15% requiring chest-tube placement.6 Other major complications are bronchopleural fistula and pulmonary infection. Bronchopleural fistula was a rare complication of thermal with 13 case reports in a literature review. Comorbidities of these patients include emphysema, chronic obstructive pulmonary disease, pulmonary bullae and bilevel positive airway pressure therapy. Among these patients, 53.8% patients had delayed massive pneumothorax, only three patients required surgery as curative treatment.7 We believe that massive pneumothorax causes respiratory failure due to tissue damage accompanied by bronchopleural fistula in our patients. Although the ablation procedure was performed with frequency and time settings as per the manufacturer's instructions, heat damage was more severe and widespread in our patient. It is possible that in older patients, the elastic properties of the lung tissue are more fragile, so the major complication of pneumothorax requiring drainage may be up to 21.1% in the elderly over 80 years old.8 Therefore, we suggest that it is probably possible to reduce the frequency and time threshold when performing MWA for the elderly with comorbidities including emphysema, chronic obstructive pulmonary disease, pulmonary bullae and bilevel positive airway pressure.
In this patient, surgical options included: open surgery or VATS. We found that open thoracotomy with a large incision can worsen respiratory failure in a very old patient. In addition, we first planned for minimal surgical intervention (pulmonary suture). So, the VATS method was more appropriate. However, the damage to the lung tissue was too large, deep and fragile, any attempt to suture or perform a wedge resection of the lung lesion failed. So, it was necessary to perform left upper lobectomy.
The local progression rates after MWA of lung malignancies vary between 0% and 34%.6 Henry Zhao and Steinke reported that in 30 patients with a median follow-up period of 56.5 months, nodal/distant progression was more common than local progression, (50% having nodal or distant metastases at follow-up vs 29% of local progression).9 This reinforces the benefit of systemic lymphatic resection in the curative surgical treatment of NSCLC, even in the early stages. In elderly patients aged 80 years and older, Han et al reported 63 patients with a median survival time 50 months with 5-year overall survival rates of 32.6%; 22.2% had local progression.8 Factors affecting the survival outcome as well as the patient’s tumour-free survival time, such as comorbidities, advanced age, poor lung function and other contraindications of surgery are additional factors to be considered when comparing the results of MWA treatment versus surgery.
Patient’s perspective
Before MWA, the patient said: ‘I am … years old this year, I just had surgery for colon cancer, the ancients have a saying ‘seventy years old is rare’, now the surgery is just painful, I don't know if I can get over it, I don't want to have surgery’.
During consultation for urgent surgery, he said: ‘Now, it’s very hard to breathe like this, so please the doctors immediately operate on me, maybe dying would be more comfortable’.
And after extubation for pulmonary lobectomy, he said: ‘Knowing this, I would have chosen surgery from the beginning’.
Learning points
The long-term results of thermal therapy for lung cancer may not be excellent, but it is still a solution that gives hope to patients, especially if they cannot or do not choose surgery.
One of the indications for microwave ablation (MWA) in lung cancer is refusal of surgery due to the high-risk factor of advancing age.
The most major complication of MWA is bronchopleural fistula due to massive thermal lung tissue damage.
Massive pulmonary necrosis and tension pneumothorax may require urgent thoracotomy or video-assisted thoracic surgery.
We suggest that it is probably possible to reduce the frequency and time threshold when performing MWA for the elderly with comorbidities including emphysema, chronic obstructive pulmonary disease, pulmonary bullae and bilevel positive airway pressure. This needs careful patient selection and vigilance following MWA in not only the elderly but also patients with comorbidities.
Ethics statements
Patient consent for publication
Footnotes
Twitter @VungoctuHmu
Contributors NTV conceived of the presented idea, reviewed the surgery, supervised the project. DTN developed the theory and performed the computations, reviewed the radiology. TTHD drafted the manuscript, reviewed the respiratory, histology and oncology. All authors reviewed and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.