Article Text

Statistics from Altmetric.com
Description
Ankle injuries, among the most widely seen emergency complaints, involve damage to the deltoid ligament of the ankle joint in 40% of the patients.1
A complex structure composed of a deep and superficial layer, the deltoid ligament, acts by opposing posterior translation and lateral displacement of the talus, thereby stabilising the ankle joint.2 Its constituent bands are highly variable, with tibionavicular ligament and tibiospring ligament of the superficial layer, and posterior tibiotalar ligament of the deep layer being the most consistently seen.2
The presentation of an acute injury to the deltoid ligament is generally pain, swelling and ecchymosis at the ankle medially, with tenderness to palpation over the affected portion of the ligament.2 However, an isolated tibionavicular component ligament injury may not present with such obvious clinical findings. Radiologically, a sign of deltoid injury is the widening of the space between the articular surfaces of the talus and medial malleolus (medial clear space).3 Injury to isolated components may not reveal such radiological features on plain radiographs. Consequently, the tears to the individual elements of the deltoid ligament may not get detected. A high index of suspicion, elucidating the mechanism of injury, focused clinical examination and complementary imaging with an MRI or operator experienced in dynamic ultrasonography (USS), is crucial to determine the extent of osseous, ligamentous and soft tissue damage.
Early identification of this uncommon pattern of injury helps in avoiding complications such as osteoarthritis, medial ankle instability and impingement syndromes.2 3
We present a case of isolated tear of the tibionavicular component of the superficial layer of the deltoid ligament presenting with medial ankle pain and normal initial radiological findings.
A young male footballer in his early 20s presented with right ankle pain, which increased on kicking a ball. He walked into the clinic with a limp. There was no obvious swelling or bruising at the ankle. Clinical examination revealed a focal tenderness at the origin of the deltoid ligament on the anterior part of the medial malleolus and a stable ankle. The ankle, subtalar and midfoot joint ranges of movements were equal to the left side. He was neurovascularly intact with normal ankle radiographs.
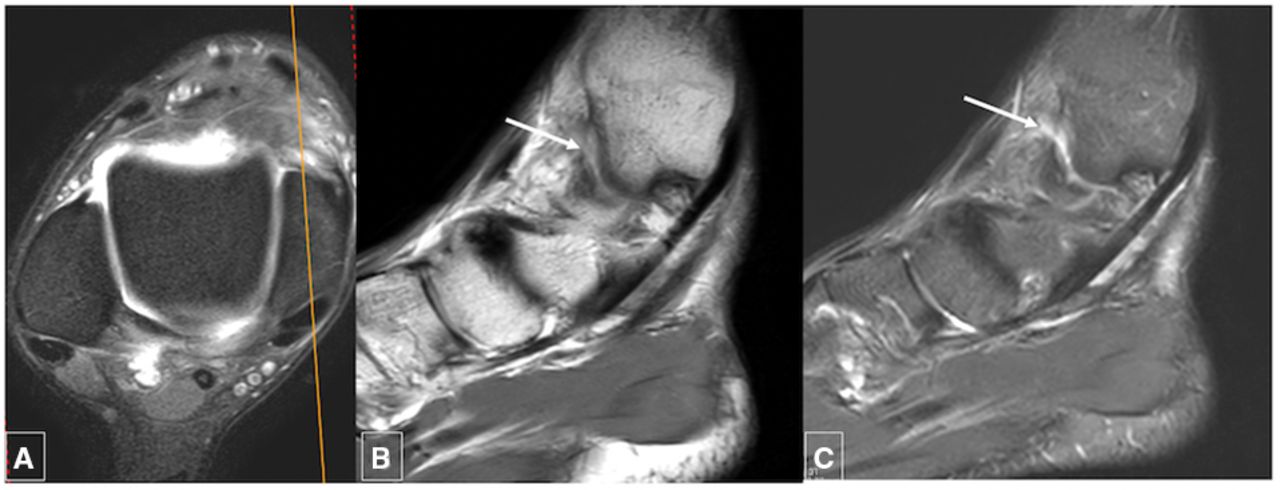
With a suspicion of injury to the underlying deltoid ligament sustained during eversion of a plantar flexed foot, an MRI was arranged. Axial and proton density fat suppressed sequences revealed features of an isolated tear of the tibionavicular component of the deltoid ligament of the ankle (figure 1). The rest of the superficial component of the deltoid ligament and the deep component of the deltoid ligament were intact. Lateral ligament complex was structurally competent.

PDFS axial (A), sagittal PD (B) and PDFS (C) MRI sequences of the ankle joint level show tear (arrows) of the tibionavicular component of the deltoid ligament at its attachment to the medial malleolus. PD, proton density; PDFS, proton density fat suppressed.
An USS-guided injection of steroid (40 mg of methylprednisolone acetate with 2% lidocaine hydrochloride) was used to treat his pain, and he was followed up with supervised, gradual return to sports (figure 2).

(A) Longitudinal and (B) oblique ultrasonography of the ankle demonstrates tear (arrows) of the tibionavicular ligament of the deltoid ligament.
This management algorithm reinforces the need to identify, localise injury with complementary imaging and thus guide effective patient treatment (figure 3).

{kind=link}
{kind=link}
{kind=link}
Schematic showing components of superficial component of deltoid ligament of the ankle joint (TCL, TNL, TS and TTL) to identify, localise injury on complementary imaging and target appropriate management. Figure drawn and prepared by senior author (RB), no permission required. TCL, tibiocalcaneal ligament; TNL, tibionavicular ligament; TS, tibiospring ligament; TTL, superficial posterior tibiotalar ligament.
Learning points
Isolated full thickness tear of the tibionavicular component of the deltoid ligament can be an unusual cause of ankle pain, presenting without features of ankle instability and normal radiographs.
The probable mechanism responsible for tear of the specific component of the deltoid ligament is due to position of the foot at the time of the injury.
A high index of clinical suspicion and complementary investigations with MRI and ultrasonography are helpful in identifying the injury to allow targeted treatment and prevent instability.
Ethics statements
Patient consent for publication
Footnotes
Contributors RB and CLK conceptualised and wrote the initial draft. KPI and DB were involved in data curation, writing the review and editing. RB and DB organised the radiological images. The schematic was prepared by RB. All authors read, validated and authorised the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.