Article Text

Statistics from Altmetric.com
Description
A woman in her 30s with stage 4 B-Raf proto-oncogene, serine/threonine kinase (BRAF) mutant melanoma with known pulmonary, intraorbital, brain and subcutaneous metastases was found to have a large mass in the right atrium (RA) on staging CT. This was new compared with a previous CT (figure 1A,B). The patient was asymptomatic from a cardiac perspective. There were no features of cardiac failure detected on examination.
{kind=link}
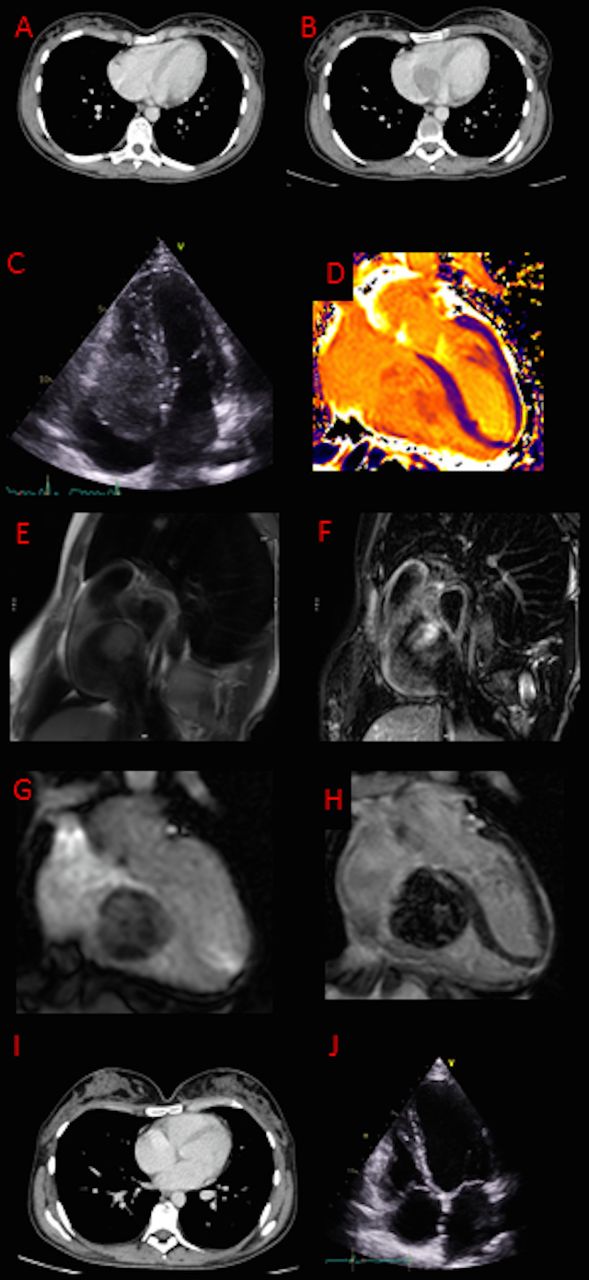
(A) CT imaging at baseline. (B) Right atrium (RA) mass on CT imaging measuring 40 mm. (C) Transthoracic echocardiogram (TTE) image demonstrating the RA mass originating from the tricuspid leaflet. (D) Cardiac magnetic resonance (CMR) showing high T1. (E) Mass was isointense on T1-weighted CMR images. (F) High T2 short tau inversion recovery (STIR) signal. (G) Contrast up-take demonstrated on first pass perfusion on CMR images. (H) Heterogeneous enhancement in the late phase following contrast. (I,J) CT and TTE images, respectively, showing resolution of the intracardiac mass following targeted therapy.
Transthoracic echocardiogram (TTE, figure 1C) subsequently demonstrated a pedunculated, mobile RA mass. The mass originated from the anterior tricuspid leaflet, measuring up to 45 mm and obstructing right ventricle inflow (peak gradient 9 mmHg). Cardiac magnetic resonance (CMR) showed the mass had a high T1 (1600 ms, figure 1D), was isointense on T1-weighted images (figure 1E), high T2 short tau inversion recovery (STIR) signal (figure 1F) and took up contrast on first pass perfusion (figure 1G). There was heterogeneous enhancement in the late phase following contrast (figure 1H).
Following a multidisciplinary meeting between the oncology, cardiology and cardiothoracic surgical teams, the decision was made for systemic immunotherapy as opposed to surgical intervention due to the high tumour burden and multiorgan involvement. Ipilimumab and nivolumab were started as first-line therapy. Due to further disease progression, second-line treatment with combination targeted therapy encorafenib (BRAF inhibitor) and binimetinib (mitogen-activated protein kinase inhibitor) was commenced. Early CT and TTE imaging following targeted therapy demonstrated almost complete resolution of the mass (figure 1I,J). Follow-up CMR was not performed, which is a limitation in the comparison of imaging pre and post therapy.
Cardiac metastasis of malignant melanoma can be intramyocardial, endocardial or pericardial.1 2 They are difficult to detect at an early stage with CT imaging and patients are often asymptomatic.3 Multimodality imaging with CMR, in particular, is useful for tissue characterisation. The T1 of the tumour is determined by the melanin content (decreasing T1 with increasing melanin). T2-weighted images are typically hyperintense and there is contrast uptake due to the vascular nature of the tumour.
Patient’s perspective
When I learnt I had stage 4 melanoma following years of having no evidence of disease, I was surprised to learn it had also spread to the heart. I had, until then, not known this was possible. Following the diagnosis, oncology requested an echocardiogram to have an input from cardiology regarding the metastasis on the heart. This led to a visit to accident and emergency department and admission to the hospital. It appeared that cardiologists were unsure about what the metastasis meant for my case and how best to respond to it. I believe the situation could have been handled better if the cardiology team had consulted with the oncology team more quickly.
Following a mixed response to immunotherapy, I was switched to targeted therapy, encorafenib (Braftovi) and binimetinib (Mektovi), which worked at an impressive speed to reduce all metastases, including the one on the heart. I have been doing better since and could not be more thankful to my oncology team.
Learning points
Malignant melanoma can lead to cardiac metastasis in some cases and a multimodality approach is often required for diagnosis. Complications include outflow tract obstruction, pericardial effusion and extracardiac thrombosis.
Multidisciplinary input is integral in the management of oncology patients with cardiac tumours.
Oncogene targeted therapy can lead to impressive early response in B-Raf proto-oncogene, serine/threonine kinase (BRAF) mutant melanoma; however, longer-term efficacy is often compromised by the development of resistance leading to tumour relapse.
Ethics statements
Patient consent for publication
Footnotes
Contributors RH and KK drafted and revised the final manuscript. KK and EN sourced and formatted the images included. NB reviewed and edited the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.