Article Text

Abstract
Primary breast lymphoma (PBL) is an uncommon type of breast malignancy. Its clinical presentation and radiographic findings are non-specific and overlap with breast carcinoma. The treatment of PBL differs significantly from breast carcinomas. Here we present a middle-aged woman who presented with an enlarging palpable right breast mass. Mammogram showed breast imaging-reporting and data system 4 findings. Breast mass biopsy pathology confirmed diffuse large B cell lymphoma. Although uncommon, clinicians should be cognisant of the possibility of PBL when patients present with a breast mass. Accurate diagnosis is essential to avoid unnecessary mastectomies.
- Breast cancer
- Malignant and Benign haematology
- Medical management
- Breast surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Primary breast lymphoma (PBL) is an uncommon type of breast malignancy, representing between 0.04% and 0.5% of all breast malignancies.1–5 It is defined as the presence of a breast lymphoma without evidence of systemic disease. It usually presents with a rapidly enlarging painless solitary mass, with or without ipsilateral axillary lymphadenopathy, which cannot be differentiated from breast carcinomas clinically. The radiographic findings of PBLs are non-specific and overlap with that of breast carcinoma. Adequate tissue sample is required for accurate diagnosis of PBL as the treatment differs significantly from breast carcinomas.
Case presentation
A woman in her early 50s presented with a 3-week history of an enlarging palpable right breast mass. She had a medical history of remote pulmonary tuberculosis. She had annual mammograms done prior with unremarkable results. She denied any history of breast implants or chest radiation. She had a remote history of oral contraceptive use. She was a non-smoker. Her maternal great aunt had breast cancer in her 50s.
The mass was first noticed during a self-breast examination 3 weeks prior to her initial visit. The patient denied B symptoms such as fever, chills, weight loss or night sweats. She also denied other breast symptoms, including breast pain, nipple discharge or skin changes. Physical examination revealed a 5×5 cm non-tender palpable mobile mass at the 12 o’clock position about 6 cm from the right nipple, firm in consistency, without skin retraction, oedema, erythema, nipple inversion or clinically palpable axillary lymphadenopathy.
Investigations
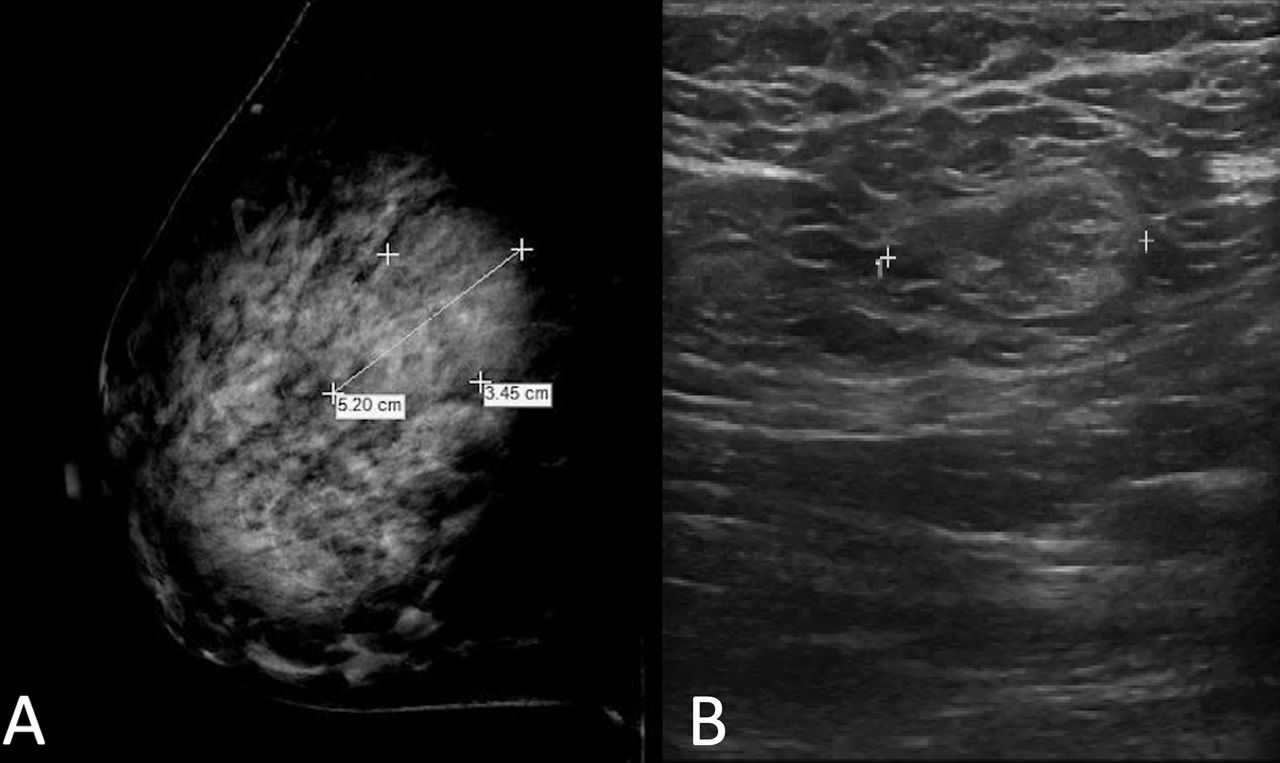
Her initial laboratory tests including complete blood count, comprehensive metabolic panel and lactate dehydrogenase were all within normal range. A mammogram was performed that demonstrated a 5.2×3.4 cm oval, equal density mass with no associated calcification in the upper quadrant 6 cm from the nipple (figure 1A). Targeted ultrasound demonstrated a 3.9×3.4×2.1 cm oval, heterogeneous predominantly hypoechoic mass with indistinct margins (figure 1B). The mass was suspicious for malignancy as breast imaging-reporting and data system 4.

Images of right breast mass. (A) Mammogram. An oval indistinct equal density mass with no associated calcifications measuring grossly 5.2×3.4 cm was visualised within the right breast at the 12 o’clock position 6 cm from the nipple. (B) Targeted ultrasound. An oval, parallel, heterogeneous predominantly hypoechoic mass with indistinct margins measuring 3.9×2.1×4.1 cm was visualised within the right breast at the 12 o’clock position approximately 5 cm, associated with faint posterior acoustic enhancement.
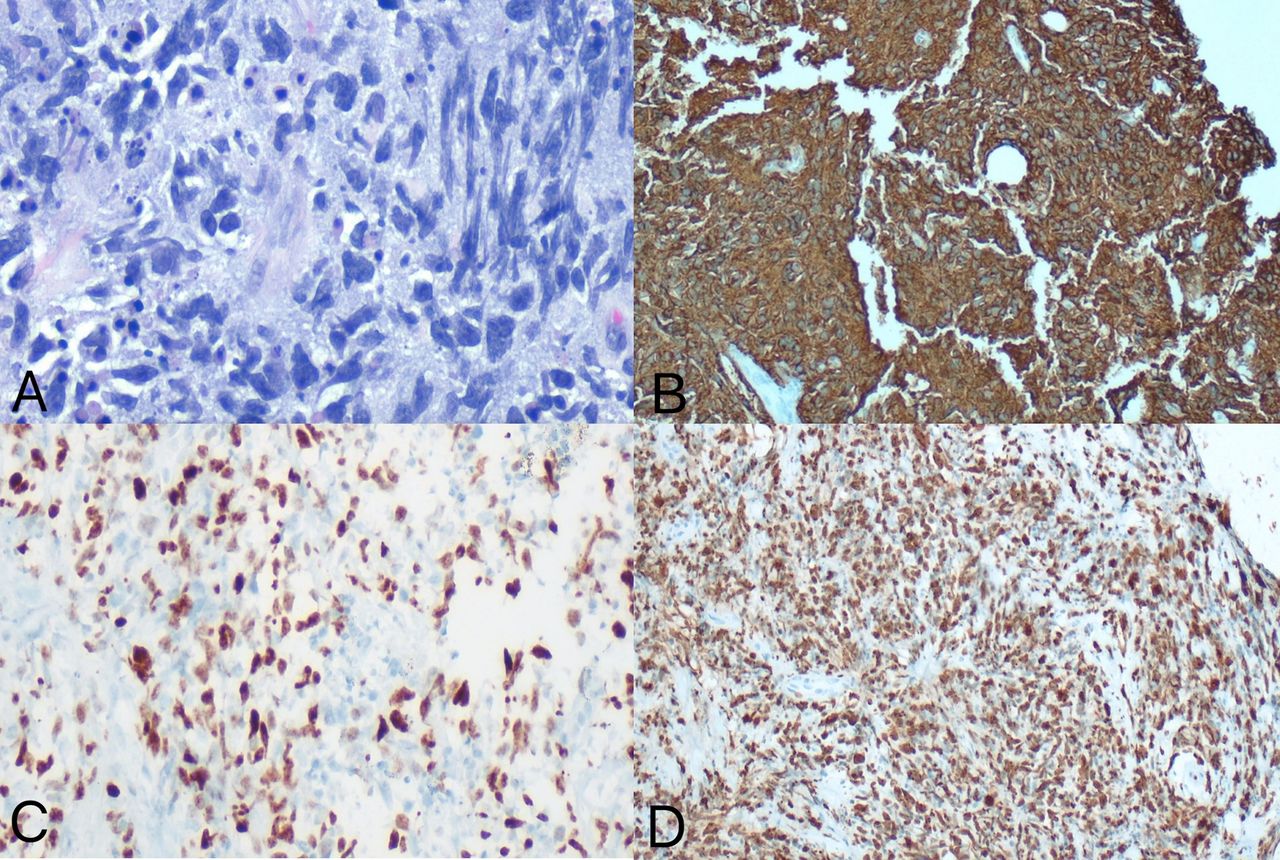
Core needle biopsy was performed. Pathology studies (figure 2) showed a high-grade diffuse large B cell lymphoma (DLBCL), non-germinal centre B cell-like (non-GCB) type. The immunohistochemical staining showed the neoplastic cells to strongly and diffusedly express CD19, CD20 and CD45, with variable (>30%–40%) expression of BCL2, BCL6, MUM1 and MYC, while negative for CD3, CD10, CD30, CD34, CD68, ALK, pancytokeratin and MART-1. On staining for Ki-67, they had a proliferation index of 90%–95%. FISH study was negative for BCL2 rearrangement, MYC rearrangement/amplification and t(8;14), but positive for BCL6 rearrangement.
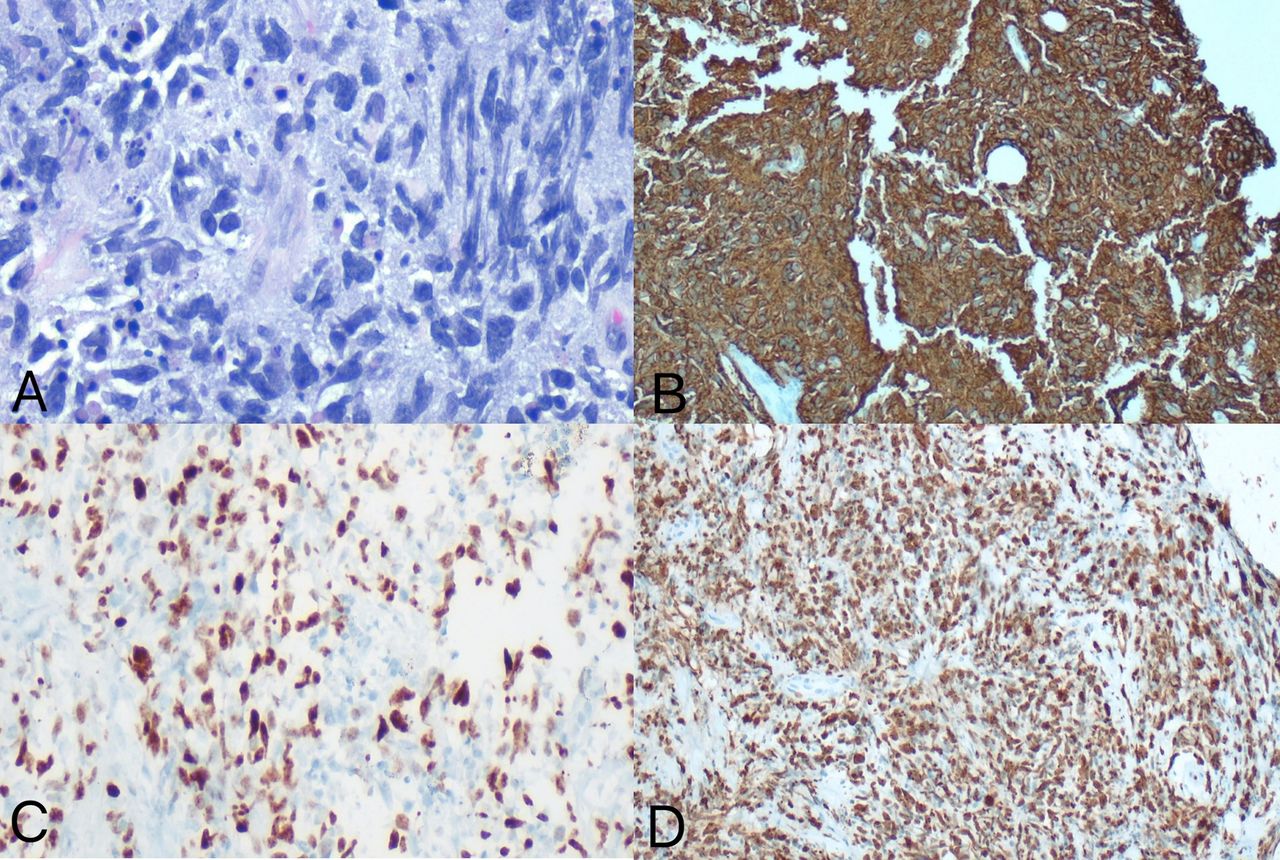
Breast high-grade diffuse large B cell lymphoma. (A) H&E stain, with markedly atypical large neoplastic cells; (B) MYC immunohistochemistry (IHC) stain, the viable neoplastic cells overexpress MYC; (C) CD20 IHC stain, the neoplastic cells are strongly positive for CD20; (D) Ki-67 IHC stain, the neoplastic cells have a high proliferation index.
Following the diagnosis, the patient was then evaluated with fluorodeoxyglucose (FDG)-positron emission tomography (PET)/CT for staging. PET/CT (figure 3A,B) showed a 4.8×3.4 cm hypermetabolic mass in the right breast, and a second FDG-avid nodule measuring up to 1.1 cm was noted between the pectoralis major and minor. In addition, FDG-avid right axillary and internal mammary lymph nodes were noted. No lesions were detected in other organs.

{kind=link}
{kind=link}
{kind=link}
(A and B) Pretreatment positron emission tomography/CT (PET/CT) demonstrates fluorodeoxyglucose (FDG) a 4.8×3.4 cm hypermetabolic mass in the right breast (solid arrow in A), FDG-avid right axillary lymph node (dashed arrow in A) and internal mammary lymph node (dashed arrow in B), and a second FDG-avid nodule measuring up to 1.1 cm between the pectoralis major and minor (solid arrow in B). (C, D and E) PET/CT after three cycles of R-CHOP therapy (R: rituximab, C: cyclophosphamide, H: doxorubicin hydrochloride, O: vincristine sulfate, P: prednisone) shows significant decrease in size and hypermetabolism of a right breast mass (solid arrows in C and E), and resolution of right axillary, subpectoral and internal mammary adenopathy. (F). PET/CT after six cycles of R-CHOP therapy shows the right breast mass continues to contract (solid arrow in F), measuring 1.2×0.7 cm, with mild accumulation of the radiotracer similar to the last examination.
Treatment
With the diagnosis of stage IIE DLBCL of the breast, non-GCB type with an international prognostic index (IPI) score of 1, the patient was started with R-CHOP treatment (R: rituximab, C: cyclophosphamide, H: doxorubicin hydrochloride, O: vincristine sulfate, P: prednisone) with regular follow-ups with her oncologist.
Outcome and follow-up
After three cycles of R-CHOP therapy, the follow-up PET/CT (figure 3C–E) showed significant decrease in the size and hypermetabolism of the right breast mass (Deauville score 3), resolution of right axillary, subpectoral and internal mammary adenopathy. The PET/CT after six cycles of R-CHOP showed additional contraction in the size of the right breast mass with residual metabolic activity (figure 3F). She then underwent consolidative radiotherapy to her right breast mass. Lumbar puncture and central nervous system (CNS) prophylaxis were recommended by her oncologist, however, the patient declined.
Discussion
The breast is an uncommon location for the development of malignant lymphoma. Breast lymphoma can be divided into PBL or secondary breast lymphoma (SBL). PBL is defined as the presence of a breast lymphoma without evidence of systemic disease. SBL is used when a systemic lymphoma concurrently or subsequently involves the breast.1 The incidence of PBL is rare, representing between 0.04% and 0.5% of all breast malignancies, approximately 1% of all non-Hodgkin’s lymphoma and 2% of extranodal lymphomas.1–5 PBLs are less common than lymphomas of other organs because the breast contains less lymphoid tissue compared with the gastrointestinal tract or the lung.6 7
PBL usually presents with a rapidly growing, painless, palpable, solitary mass and relatively mobile, with or without ipsilateral axillary lymphadenopathy, mimicking a breast carcinoma.7 8 It occurs almost exclusively in women in the fifth to sixth decade of life.2 6 7 9 The right breast is the most frequently involved site.6 7 It has a predilection for the superior quadrant.10–12 Unilateral breast involvement is more common while approximately 10%–11% of patients may have bilateral disease.6 11 12 The usual B symptoms associated with lymphoma, such as weight loss, fever and night sweats, are rarely seen in PBLs.6 12 PBLs cannot be differentiated from breast carcinomas clinically. Compared with breast carcinomas, PBLs tend to be larger and associated symptoms of skin retraction, erythema, nipple discharge and peau d’orange are uncommon.2 8
B cell breast lymphomas are more common than the T cell type.4 9 PBLs have diverse histological subtypes. Approximately one-half of PBLs are DLBCL,13 followed by follicular lymphomas and extranodal marginal zone lymphomas. Patients with PBLs are thought to have a similar prognosis to patients with lymphomas of the same histology types and stages arising at other sites.8 10 As for SBL, the prognosis depends on the stage of the primary malignancy.6
Early stage, low histological grade and a favourable IPI are all favourable prognostic factors for PBLs.2 4 DLBCL has a worse prognosis compared with other subtypes.
The imaging findings of PBL are non-specific and resemble those of breast cancer. No single imaging finding is considered pathognomonic. The image findings of PBL also overlap with SBL.2 6 The most frequent findings of PBL on mammography are a single, relatively well-circumscribed uncalcified mass.2 6 8 It is less common for PBL masses to have microcalcifications, spiculations, irregular borders or architectural distortion in the surrounding tissue. In a study performed by Sabate et al, 12.5% PBL masses had well defined, mimicking benign lesions.14 The ultrasound and MRI manifestations of PBLs are also variable and non-specific.10 PET/CT plays an important role in the management of PBL, including staging, treatment response evaluation and recurrence detection.6
PBL is often diagnosed based on histological findings since the imaging findings of PBL are non-specific and overlap with other malignant and even benign breast tumours.12 In 1972, Wiseman and Liao proposed the following criteria for PBL: adequate tissue specimen for pathology, lack of a prior diagnosis of an extramammary lymphoma, close anatomical proximity of mammary tissue and lymphomatous tissue, and no synchronous disseminated disease (except for the ipsilateral axillary nodal involvement).15 All lymphomas involving the breast but not meeting all the above criteria are considered as SBL.7
Excisional biopsy and core biopsy are the preferred techniques for adequate tissue acquisition, with the latter being preferred given its minimally invasive nature. Fine needle aspiration (FNA) is not recommended. Although it may differentiate lymphoma from breast carcinoma, the FNA sample lacks architectural detail necessary to accurately classify lymphoma subtypes.1
The treatment of PBL differs from breast carcinoma in that the emphasis is on systemic chemotherapy.4 Although the management of PBL has not been standardised yet, a diagnostic biopsy followed by chemotherapy and radiotherapy is recommended.9 Existing literature has demonstrated that mastectomy results in higher mortality and poorer prognosis.16 PBL is a haematological malignancy, and its pathogenesis and progression differ significantly from breast carcinoma. Like lymphoma that occurs at extramammary sites, local surgical resection would not be as beneficial for tumour control as systemic therapy. Therefore, radical surgery should be avoided in PBL. For patients with PBLs who undergo surgical intervention for initially presumed breast carcinoma, the follow-up comprehensive treatment including chemotherapy and radiotherapy should be administered promptly following surgery.1 13 16 17 It is important to differentiate PBL from breast carcinoma based on core-needle biopsy to avoid unnecessary radical surgery in PBL.
DLBCL is the most common histopathological subtype of PBL. Due to its worse prognosis compared with other subtypes and rapid progression, prompt treatment is indicated. Chemotherapy is an effective treatment for primary breast DLBCL. R-CHOP remains the first-line treatment regimen.16 This may be followed by radiotherapy, with most of the data showing this combined modality can improve survival and reduce local recurrence.18 19 CNS prophylaxis in primary breast should be considered given higher CNS recurrence rates in primary breast DLBCL.12 13 16
In conclusion, although the clinical presentation and imaging findings of PBL are non-specific and overlap with that of breast carcinoma, their management is vastly different. Clinicians should be cognisant of the possibility of PBL when patients present with a breast mass. Accurate diagnosis is essential to avoid unnecessary mastectomies.
Patient’s perspective
I’ve never heard about breast lymphoma in the past. I have friends who are fighting with breast cancer and had their breasts removed by surgeons. When my biopsy result came out, I was scared and I was concerned when my doctor said the treatment was not surgical removal. Fortunately, my breast mass shrunk quickly after the chemotherapy.
Learning points
Although the clinical presentation and imaging findings of primary breast lymphoma are non-specific and overlap with that of breast carcinoma, their management is vastly different.
When a breast mass is discovered, breast lymphoma should always be included in the differential diagnosis.
Accurate diagnosis with adequate tissue biopsy and histopathology is essential to avoid unnecessary surgical therapy and optimise lymphoma treatment.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors MG and JL: conception, literature review and drafting of the manuscript. RG and GT: critical revision of the manuscript and final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.