Article Text

Statistics from Altmetric.com
Description
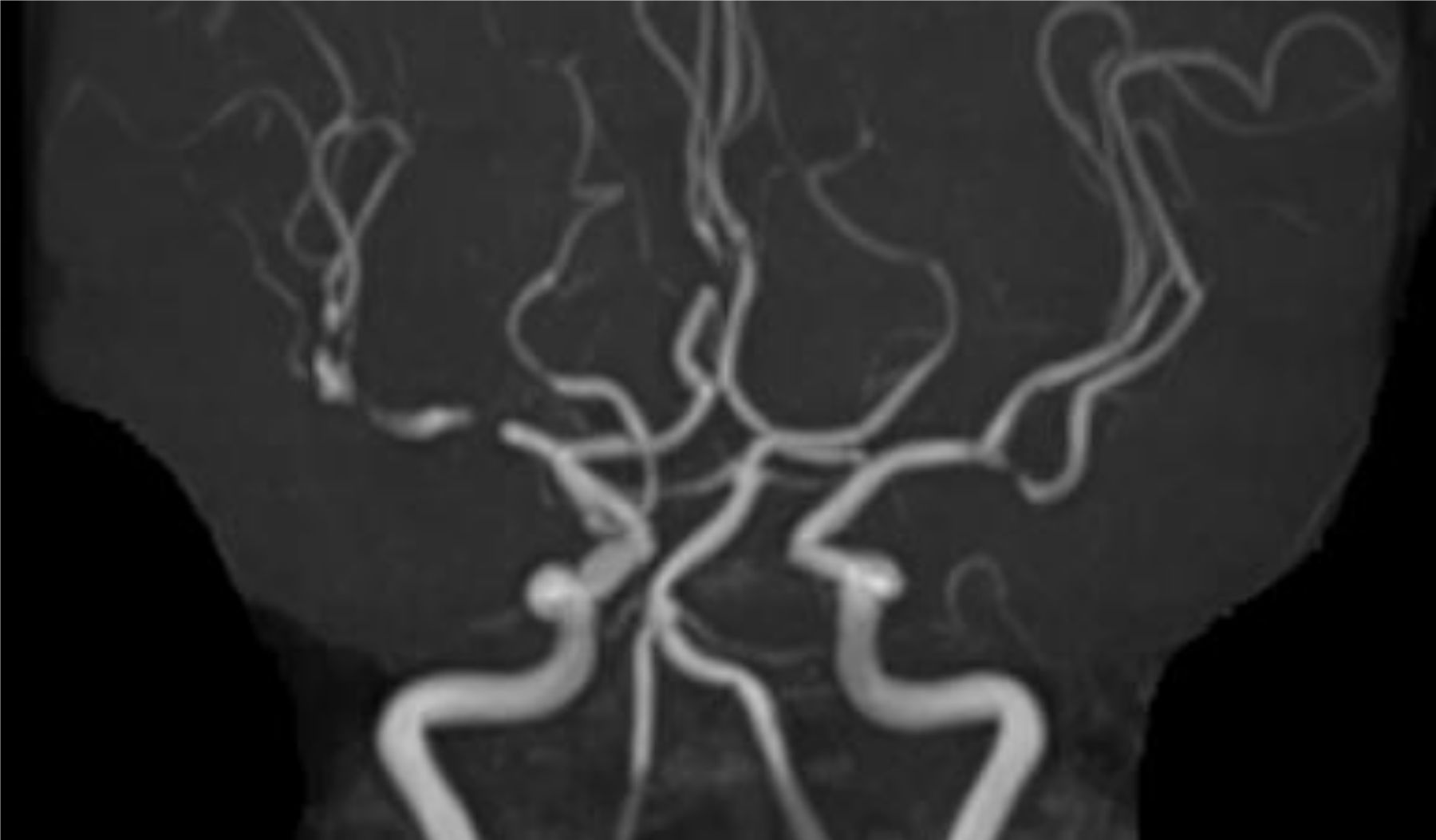
An elderly Japanese woman in her 80s had left hemiparesis and hemiparesthesia, which were accompanied by a newly developed temporal headache that had lasted for 2 weeks. Since these symptoms were not severe, she was not admitted to a hospital for care. She has a history of well-controlled hypertension and bronchial asthma. MRI revealed a subacute right cerebral infarction with multiple severe stenosis of the bilateral middle cerebral arteries (MCAs) (figure 1A), even though they were intact when the MRI was performed, which is, by chance, due to the detailed examination for the numbness of the extremities and dizziness 3 years before (figure 1B). Simultaneously, prolonged erythrocyte sedimentation rate (ESR) elevation (131 mm/hour) also coexisted. Serum myeloperoxidase and proteinase 3 antineutrophil cytoplasmic antibody were both negative and no other vascular complication as well as malignant tumour or signs of infectious diseases was shown by whole body contrast enhanced CT, however, the biopsy of the superficial temporal artery revealed inflammatory cell infiltration into the tunica media and thickening of the tunica intima (figure 2), which were consistent with giant cell arteritis (GCA). According to the American College of Rheumatology 1990 criteria for the classification of GCA,1 the diagnosis of GCA and intracranial GCA (IC-GCA) was made and the patient was administered 25 mg per day of oral prednisolone (0.5 mg/kg/day) in addition to antiplatelet therapy. After the initiation of prednisolone, the ESR promptly improved to 20 mm/hour, and the follow-up MRI exhibited an improvement in the MCA stenosis (figure 3) without any recurrence of infraction up to 3 months later.

MRI revealed multiple severe stenosis of the bilateral middle cerebral artery (A; arrow head). It was intact 3 years before (B).

Superficial temporal artery biopsy revealed inflammatory cell infiltration into the tunica media and thickening of the tunica intima, which are findings consistent with those of giant cell arteritis.
{kind=link}
{kind=link}
{kind=link}
After the initiation of prednisolone, the stenosis of the middle cerebral artery improved, and there was no recurrence of infraction up to 3 months later.
The prevalence of GCA in Japan is reported to be extremely low (1.47 per 100 000 population) compared with that in other countries.2 Although GCA is sometimes involved in IC arteries, such as the internal carotid artery or vertebral artery, occurrences in the MCA are rarely reported. IC-GCA is difficult to diagnose when the patient initially presents with a stroke,3 however, it is reported to be associate with significant mortality and more prevalent than currently recognised.4 In this case, of course traditional stroke such as atherothrombotic infarction could not be ruled out, however, we concluded that it was more reasonable to explain newly developed bilateral multiple stenosis of MCA if the GCA was involved. Here, we report the unique MRI finding of bilateral MCA stenosis and emphasise the risk of potential underlying GCA among stroke patients, especially when the condition is accompanied by unexplained inflammation or headache.
Learning points
Intracranial giant cell arteritis (GCA) is difficult to diagnose when the patient initially presents with a stroke.
Underlying GCA should be considered among stroke patients, especially when the condition is accompanied by unexplained inflammation or headache.
Ethics statements
Patient consent for publication
Footnotes
Contributors All authors saw tha patient. AK wrote the manuscript and YO, KD, and HW revised it.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.