Article Text

Statistics from Altmetric.com
Description
A unilocular radiolucency involving the mandible poses a diagnostic enigma in the case of asymptomatic patients. A plethora of pathologies such as giant cell lesions, odontogenic cysts or tumours and vascular tumours are often considered while investigating an incidentally found mandibular radiolucency presenting no clinical signs or symptoms. However, tumours such as schwannoma are often neglected.
Schwannomas (neurilemmomas) are benign, slow growing nerve sheath tumours arising from the Schwann cells that cover the myelinated nerve fibres.1 First described by Virchow in 1908 and later named as neurilemmoma by Verocay in 1910, schwannomas are usually encapsulated. A total of 88 cases of intraosseous schwannomas of the jaws have been reported in literature. The mandible is the most common site, accounting for 85% of the cases.2 The common symptoms associated with intraosseous schwannomas include tooth mobility and displacement, swelling, pain and paraesthesia, which are seen in 84% of the cases at the time of diagnosis.2 In almost all the cases, histopathological analysis gives a definitive diagnosis of schwannoma. The histopathological features include encapsulation, presence of well-differentiated cells with nuclear palisading surrounding Verocay bodies (Antoni type A tissue) and poorly organised cells with thickened blood vessels (Antoni type B tissue).3 Since schwannomas are well encapsulated, surgical enucleation remains the treatment of choice, with a recurrence rate of 8%.2 Postoperative paraesthesia was noted in 8% of the cases and there is lack of evidence regarding the return of sensation following paraesthesia.2
A young woman reported to the dental office with pain in her lower left back tooth region. No relevant medical history was presented. Intraoral examination revealed an impacted mandibular third molar on the left side with no visible facial swelling. An orthopantomogram was advised for evaluation of the impacted tooth and an incidental finding of a well-defined radiolucency measuring about 1 cm × 1 cm in diameter involving the right body of the mandible lying directly over the inferior alveolar canal was detected from the orthopantomogram (figure 1A). A CT was obtained to determine the exact boundaries and the nature of the lesion. A provisional diagnosis of giant cell tumour, odontogenic tumour and peripheral nerve sheath tumour was made. Under general anaesthesia, an intraoral muco-vestibular incision was placed and surgical enucleation of the lesion along with a part of the inferior alveolar nerve was performed (figure 1B). Classic Antoni A and Antoni B areas with Verocay bodies (figure 2A) were noted in the histopathological sections and a strong positivity for S100 staining was also observed (figure 2B), confirming the diagnosis of Schwannoma. A 1 year follow-up revealed no signs of recurrence and partial return of sensation to the right-side lower lip.

(A) Orthopantomogram indicating a well-defined radiolucency measuring 1 cm x 1 cm in relation to the apex of mandibular right first molar tooth. The lesion can be seen involving the inferior alveolar nerve canal. (B) Intraoperative image depicting the defect postenucleation of the lesion.
{kind=link}
{kind=link}
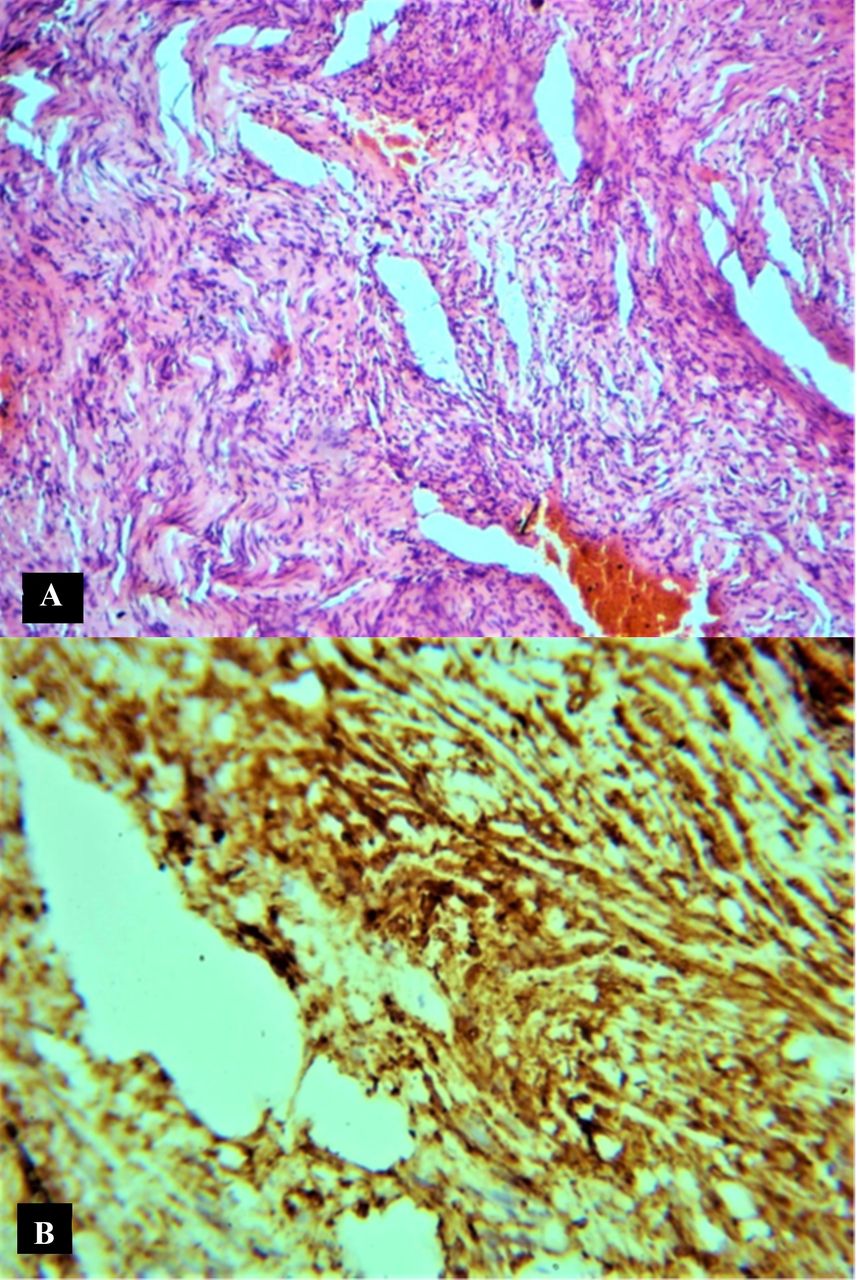
(A) Photomicrograph demonstrating Antoni A areas, Verocay bodies and Antoni B areas. (B) Immunohistochemical analysis depicting positivity for S100 protein confirming the diagnosis of schwannoma.
Patient’s perspective
On a lighter note, I am thankful to my wisdom teeth for giving me the trouble. Else this tumour would not have been diagnosed until late. I am happy the doctors got rid of the tumour this early and my lip sensation has returned to around 70% of the presurgery levels.
Learning points
Radiographic imaging can play a pivotal role in identifying rare intraosseous pathologies, especially in the absence of clinical signs or symptoms.
Schwannomas can be considered in the differential diagnosis of unilocular, well-circumscribed lesions centred on the inferior alveolar nerve.
Early management of these benign neural tumours may reduce complications such as bony erosion and loss of teeth.
Ethics statements
Patient consent for publication
Footnotes
Contributors RR is the pathologist who diagnosed this case and contributed to manuscript preparation. PS is the sole operating surgeon and also contributed to manuscript preparation. TMD contributed to the preparation of the manuscript and final language editing. MVJ contributed to the manuscript preparation and patient care. RR and PS contributed equally to the management of this case and manuscript preparation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.