Article Text

Statistics from Altmetric.com
Description
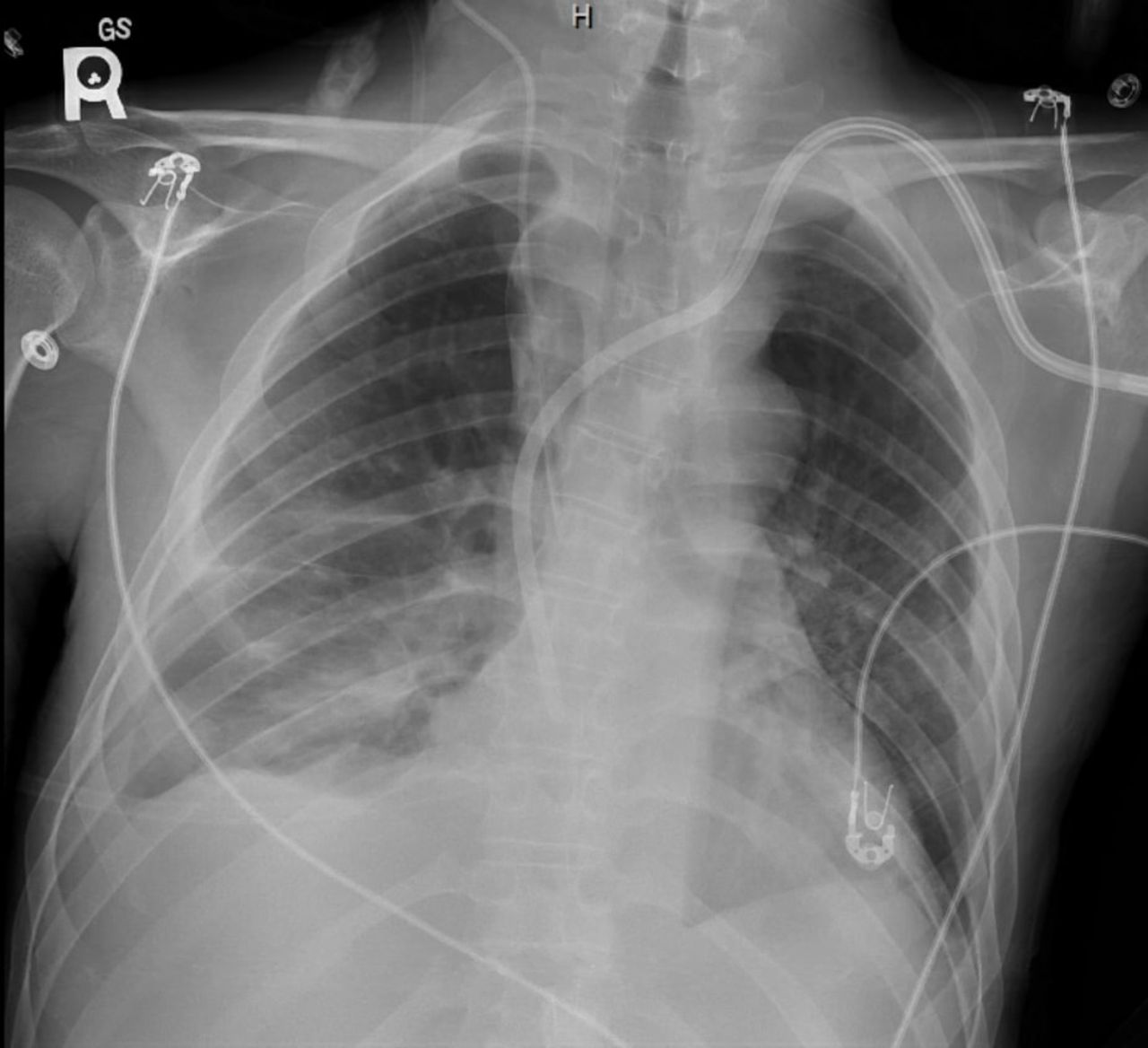
A young man in his 20s with a history of systemic lupus erythematosus (SLE) was admitted a month ago for acute kidney injury secondary to lupus nephritis. He received pulse corticosteroids and two doses of cyclophosphamide a month apart and required maintenance haemodialysis. He presented again with shortness of breath and haemoptysis. He was tachypneic with a respiratory rate of 30/min, hypoxaemic with an O2 saturation of 72%, and required supplemental O2 with a non-rebreather mask. He had not missed any dialysis sessions in the 1 week since discharge. In the emergency department, the initial laboratory workup was significant for leucocytosis with white cell count of 17×109 /L, and normocytic anaemia with haemoglobin of 90 g/L, his chest X-ray (CXR) showed complete opacification of the right hemithorax and extensive left lung opacities (figure 1). CT chest without contrast showed extensive bilateral infiltrates and a moderately large right effusion with right lower lobe atelectasis (figure 2). Right pleurocentesis was done, with the removal of 1 L of pleural fluid, which was transudative.

CXR showed complete opacification of the right hemithorax and extensive left lung opacities. CXR, chest X-ray.

CT showed large right pleural effusion and extensive left lung opacities.
He was placed on BiPAP but required intubation for continued hypoxaemia and increased work of breathing. Bronchoscopy revealed blood clots at the carina and on the right and left main bronchi. On bronchoalveolar lavage (BAL), bloody non-clearing secretions were obtained; these findings were consistent with diffuse alveolar haemorrhage (figure 3). He was given 1 g methylprednisolone empirically for lupus pneumonitis. Viral panel done on the BAL was positive for varicella-zoster virus (VZV) PCR. He was diagnosed with VZV pneumonitis, corticosteroids were quickly tapered down, and acyclovir 5 mg/kg intravenous was started daily for 7 days. His follow-up CXR (figure 4) showed marked improvement of pulmonary infiltrates; he was extubated and discharged on prophylactic acyclovir and trimethoprim-sulfamethoxazole.

Non-clearing bloody secretions obtained by BAL. BAL, bronchoalveolar lavage.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Follow-up CXR showed marked improvement of pulmonary infiltrates. CXR, chest X-ray.
Alveolar haemorrhage is a rare but life-threatening presentation in patients with SLE.1 It is usually attributed to lupus pneumonitis; however, when a patient has been on long-standing immunosuppressive therapy, an infectious aetiology should be considered, and BAL with cultures and viral PCR should be performed. VZV pneumonia is usually associated with underlying medical conditions or immunosuppression, but it can occur in healthy young individuals, especially pregnant women. Respiratory disease severity, early bacterial coinfection and other organ failures are independent risk factors for morbidity and mortality. Treatment is mainly supportive with antiviral therapies. Adjunctive corticosteroid therapy is controversial.2
Learning points
Varicella-zoster virus pneumonia is usually associated with underlying medical conditions or immunosuppression, but healthy young individuals also develop this pneumonia.
Respiratory disease severity, early bacterial coinfection and other organ failures on intensive care unit admission are independent risk factors for invasive mechanical ventilation.
The mainstay of treatment is supportive treatment and antiviral therapy while the use of adjunctive steroid therapy is controversial.
Ethics statements
Patient consent for publication
Footnotes
Twitter @M_H_Abdelnabi
Contributors NE and MA wrote the manuscript, KN, JP revised the manuscript. All the authors red and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.