Article Text

Statistics from Altmetric.com
Description
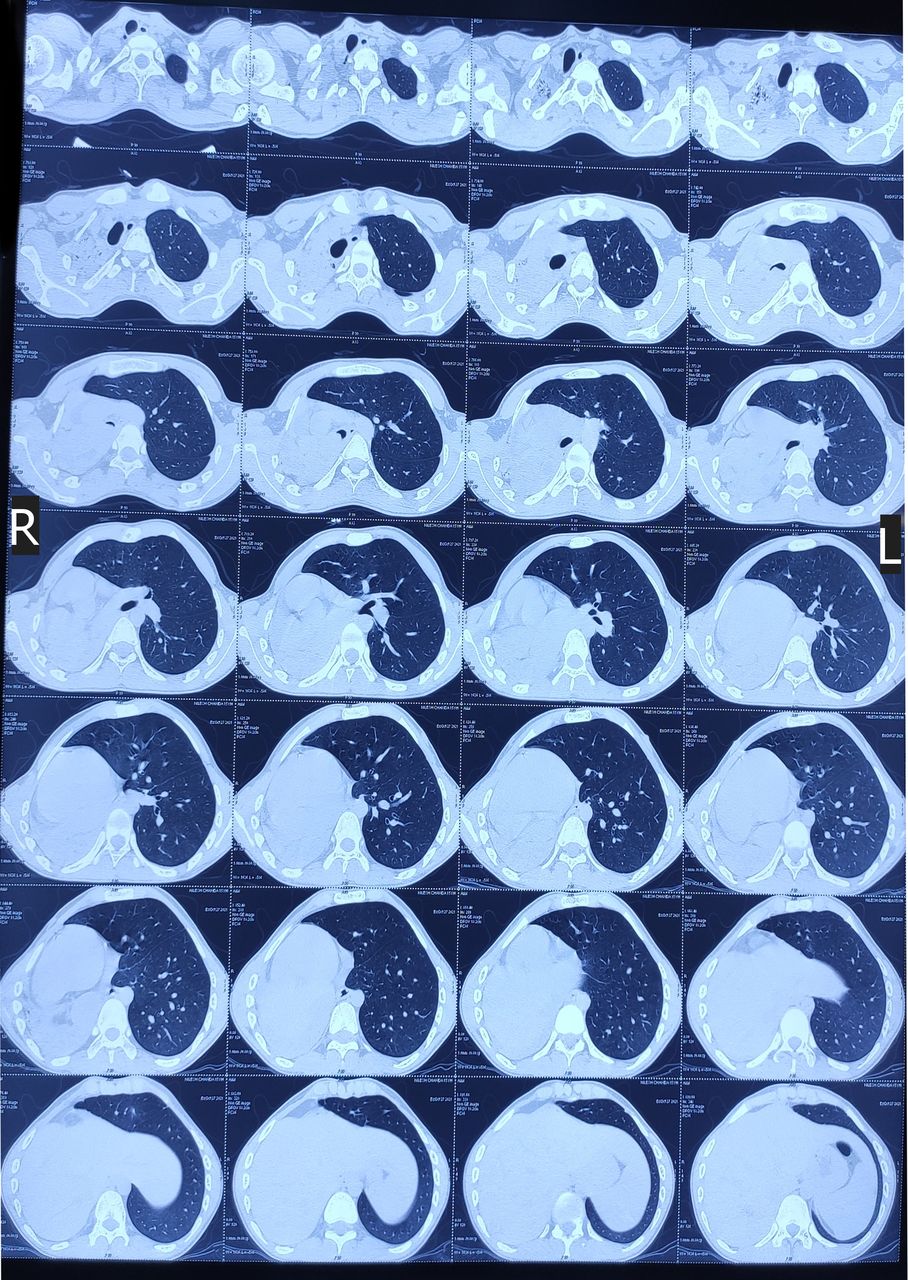
A postpneumonectomy-like syndrome is a rare condition that arises due to unilateral lung pathology that subsequently leads to severe lung volume loss resulting in mediastinal shift and herniation of the healthy lung into the contralateral hemithorax, mimicking the condition after a pneumonectomy surgery.1 An adolescent male with a chief complaint of haemoptysis, cough with expectoration and breathlessness for 2 years was admitted to the surgery department and sent for preanaesthetic evaluation at a preanaesthesia check-up clinic. General physical examination revealed external deformity of the chest wall with a rib cage bulge on the left side. The auscultation findings were decreased breath sound but a better appreciation of cardiac sounds on the right side of the chest. The patient had a resting heart rate of 92 beats per minute, blood pressure of 110/83 mm Hg and respiratory rate of 14–16 breaths per minute. The patient had dyspnoea of grade 1 on the modified Medical Research Council (mMRC) scale. The radiological examination revealed complete opacity on the right side with a barely visible lung field and deviation of the trachea to the right side on the chest X-ray (figure 1). Contrast-enhanced CT of the chest showed a well-defined lobulated homogeneously enhancing soft tissue density lesion measuring 3.2×3.1×2.5 cm in the tracheal lumen at the level of carina extending into the right main bronchus causing complete obliteration and collapse of the right lung resulting in a massive mediastinal shift towards the right side and dextroversion of cardiac apex with compensatory hypertrophy of left lung (figure 2). Lung perfusion scintigraphy with Tc-99m macroaggregated albumin scintigraphy (Tc-99 MAA) showed a well-perfused left lung and a very faintly visualised right lung.

Chest X-ray showing opacity with barely visible right lung field and tracheal deviation to the right side.

Contrast-enhanced CT chest coronal sections showing a mass arising in the tracheal lumen at the level of carina and extending into the right main bronchus causing complete obliteration and collapse of the right lung resulting in a massive mediastinal shift towards the right side and dextroversion of cardiac apex with compensatory hypertrophy of the left lung.
Flexible video broncoscopy showed vascular mass arising from the posterior wall of the lower trachea with a broad base, completely occluding the opening of the right main bronchus (figure 3). The video broncoscope could not progress through the same and tracheal carina could not be visualised. As the biopsy from the mass could not be taken due to the highly vascular nature of the mass, a provisional diagnosis of carcinoid tumour was made based on clinical, radiological and endoscopic findings.2–4 Tracheobronchial tumours are very rare and represent only 0.6% of lung tumours and carcinoids constitute 0.4%–3% of all lung malignancies.4 5 The patient was scheduled for right pneumonectomy with carinal resection and tracheal reconstruction after consensus among clinical team members, the patient and his guardians. The previous literature has also reported a similar case that also required pneumonectomy.6

{kind=link}
{kind=link}
{kind=link}
Flexible video bronchoscopy images showing mass arising from (A) posterior wall of the lower trachea with a broad base, (B) completely occluding opening of right main bronchus and (C) left main bronchus free of tumour.
A wide range of symptoms may be present in these patients, from no symptoms to severe breathlessness, stridor, syncope or dysphagia.6 A herniated lung into the contralateral hemithorax may lead to rotation of the heart and great vessels, compression of the trachea and main stem bronchi, and airway stenosis or oesophageal compression.7 These conditions may contribute to a low cardiorespiratory reserve, decreased exercise tolerance and abnormal pulmonary function. A preoperative cardiovascular risk assessment and optimisation with preoperative pulmonary rehabilitation are recommended.8 A thorough preanaesthetic evaluation should include a detailed history, meticulous clinical examination, pulmonary function tests and appropriate use of imaging modalities for perioperative risk assessment. This approach in turn helps in better perioperative optimisation and management and good postoperative outcomes.9
Learning points
Radiological, endoscopic and nuclear imagings play a crucial role in the assessment of such selected patients.
Long-standing disease process leads to various compensatory physiological changes in the body that needs to be assessed properly and patients to be optimised adequately before the surgery.
Careful clinical examination and utilisation of appropriate imaging modalities help anaesthesiologists to make patient-tailored plans for perioperative management.
Ethics statements
Patient consent for publication
Footnotes
Contributors RS: concept, design, idea to publish, manuscript editing. KSR: manuscript editing, data collection, final approval. TM: data collection, final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.