Article Text

Abstract
A woman in her 50s with a background of chronic obstructive pulmonary disease secondary to smoking presented with intermittent chest tightness, dyspnoea and vomiting for 4 days. A presumed diagnosis of acute coronary syndrome (ACS) was made based on dynamic ischaemic ECG changes and elevation in high-sensitivity cardiac troponin T levels. She underwent emergent coronary angiography which demonstrated mild coronary artery disease with left ventriculography suggestive of mid-wall variant Takotsubo cardiomyopathy. Thyroid function tests performed to investigate sinus tachycardia were consistent with hyperthyroidism, and her thyroid-stimulating hormone receptor antibody was elevated. A diagnosis of thyroid storm was made in the setting of a newly diagnosed Graves’ disease and the patient was subsequently commenced on guideline-based therapy. This case demonstrates that Takotsubo cardiomyopathy, a mimic of ACS, is a possible complication of thyroid storm and therefore hyperthyroidism should be considered in the list of differentials in patients presenting with Takotsubo cardiomyopathy.
- Cardiovascular medicine
- Thyroid disease
- Clinical diagnostic tests
- Thyrotoxicosis
- Heart failure
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Takotsubo cardiomyopathy presentation is a mimic of acute coronary syndrome (ACS).1 Abnormal thyroid hormone concentrations have been reported in patients with Takotsubo cardiomyopathy, but the causal association has not been fully established.2 3 Thyroid hormone excess leads to increased cardiac stimulation, manifesting with tachyarrhythmia, inotropy and hypermetabolism, and should be investigated in patients presenting with Takotsubo cardiomyopathy.4 5
Case presentation
A woman in her 50s was brought to the emergency department by ambulance with a 4-day history of worsening intermittent chest tightness, dyspnoea, vomiting and lethargy, with a background history of 30-pack-year smoking. She was treated by the paramedics with 10 mg of nebulised salbutamol, 500 μg of nebulised ipratropium bromide and 8 mg of intravenous dexamethasone for presumed exacerbation of chronic obstructive pulmonary disease (COPD). In view of a possible diagnosis of ACS, she was administered sublingual glyceryl trinitrate and a loading dose of aspirin (300 mg) in the emergency department. Prior to symptom onset, the patient was well with no recent intercurrent illnesses nor previous hospitalisations. Her medical history was significant for COPD, maintained on tiotropium bromide (Spiriva) and as-required inhaled salbutamol, chronic lower back pain and anxiety. She had a strong family history of ACS, with no family history of any thyroid disease or autoimmune disease. She lived independently at home with her son.
On initial examination the patient was normotensive but remained persistently tachycardic, with a heart rate ranging from 110 to 130 beats per minute, with no altered mental status. There was no audible wheeze nor evidence of fine bibasal/diffuse crepitations on auscultation of her lungs. Heart sounds were dual, with no audible murmurs, additional heart sounds or pericardial rub. There was a fine tremor that was initially attributed to salbutamol use. There was no evidence of thyroid acropachy, lid lag or lid retraction, or exophthalmos. Her thyroid was slightly enlarged but non-tender on palpation. Proximal muscle strength was 5 of 5 bilaterally, with bilateral brisk patella and Achilles reflexes.
Initial investigations demonstrated mild neutrophilia (8.5×109/L; normal ~2.0–8.0×109/L) and lymphopaenia (0.6×109/L; normal 1.0–4.0×109/L), with a C reactive protein level of 6 mg/L (normal <6 mg/L). Thyroid function studies were performed. Chest X-ray demonstrated clear lung fields, with no evidence of lung collapse or consolidation. The patient was admitted and initially managed for non-infective exacerbation of COPD. A high-sensitivity cardiac troponin T (hs-cTnT), which was performed due to presentation with chest tightness, was elevated at 151 ng/L (normal <16 ng/L). Initial ECG on presentation demonstrated sinus tachycardia with normal axis without ST segment elevation or depression (figure 1A). The patient was commenced on dual antiplatelet therapy that included aspirin 100 mg daily, ticagrelor 90 mg two times per day, rosuvastatin 40 mg daily and therapeutic enoxaparin for management of a non-ST-elevation myocardial infarction (NSTEMI).

(A) ECG taken on presentation demonstrating sinus tachycardia. (B) ECG demonstrating dynamic ST changes in leads V1–V2. The arrows indicate J-point elevation above the isoelectric line in leads V1–V2.
Prior to planned coronary angiography, the patient developed acute-onset dyspnoea with associated chest tightness. A repeat ECG was performed and demonstrated sinus tachycardia with dynamic ST elevation in V1–V2 (figure 1B). Emergent coronary angiography was performed and demonstrated mild coronary artery disease.
Following the patient’s angiogram, a single episode of atrial flutter was noted and was managed with intravenous digoxin and intravenous amiodarone, with subsequent reversion to sinus rhythm. No further episodes of atrial flutter occurred.
Investigations
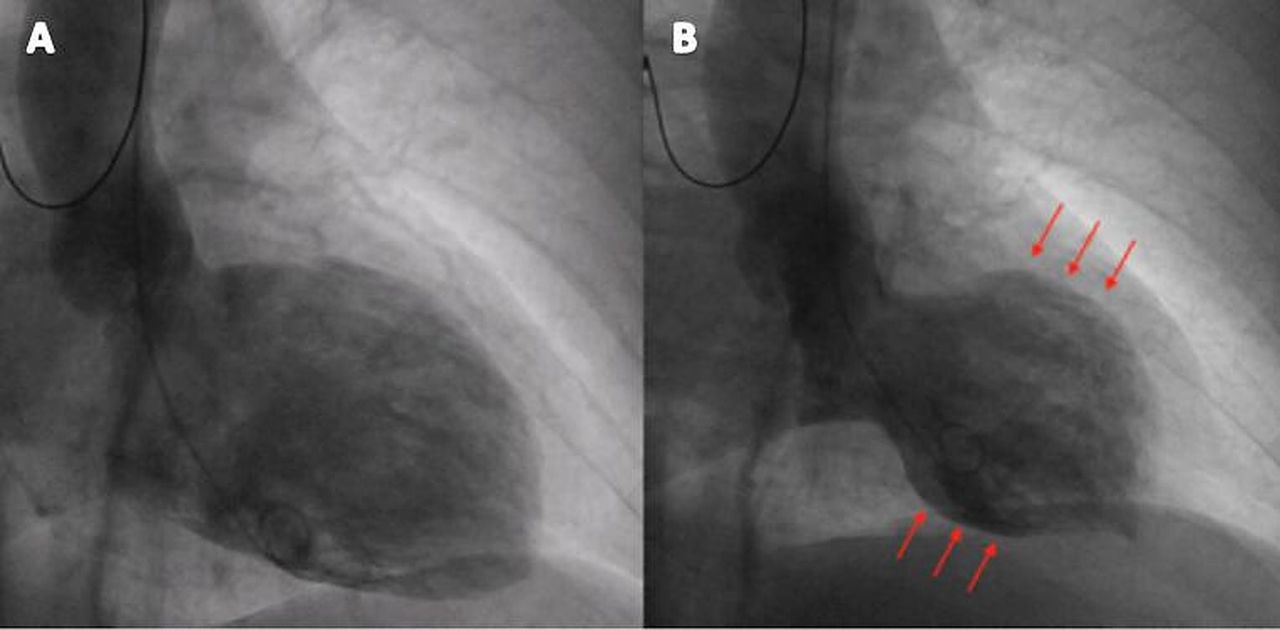
An emergent coronary angiogram was performed which demonstrated only mild coronary artery disease (video 1). Left ventriculography showed a markedly dilated left ventricle with preserved contraction of the basal and apical wall segments suggestive of mid-wall variant Takotsubo cardiomyopathy (video 2, figure 2A,B).
Disclaimer: this video summarises a scientific article published by BMJ Publishing Group Limited (BMJ). The content of this video has not been peer-reviewed and does not constitute medical advice. Any opinions expressed are solely those of the contributors. Viewers should be aware that professionals in the field may have different opinions. BMJ does not endorse any opinions expressed or recommendations discussed. Viewers should not use the content of the video as the basis for any medical treatment. BMJ disclaims all liability and responsibility arising from any reliance placed on the content.
Disclaimer: this video summarises a scientific article published by BMJ Publishing Group Limited (BMJ). The content of this video has not been peer-reviewed and does not constitute medical advice. Any opinions expressed are solely those of the contributors. Viewers should be aware that professionals in the field may have different opinions. BMJ does not endorse any opinions expressed or recommendations discussed. Viewers should not use the content of the video as the basis for any medical treatment. BMJ disclaims all liability and responsibility arising from any reliance placed on the content.
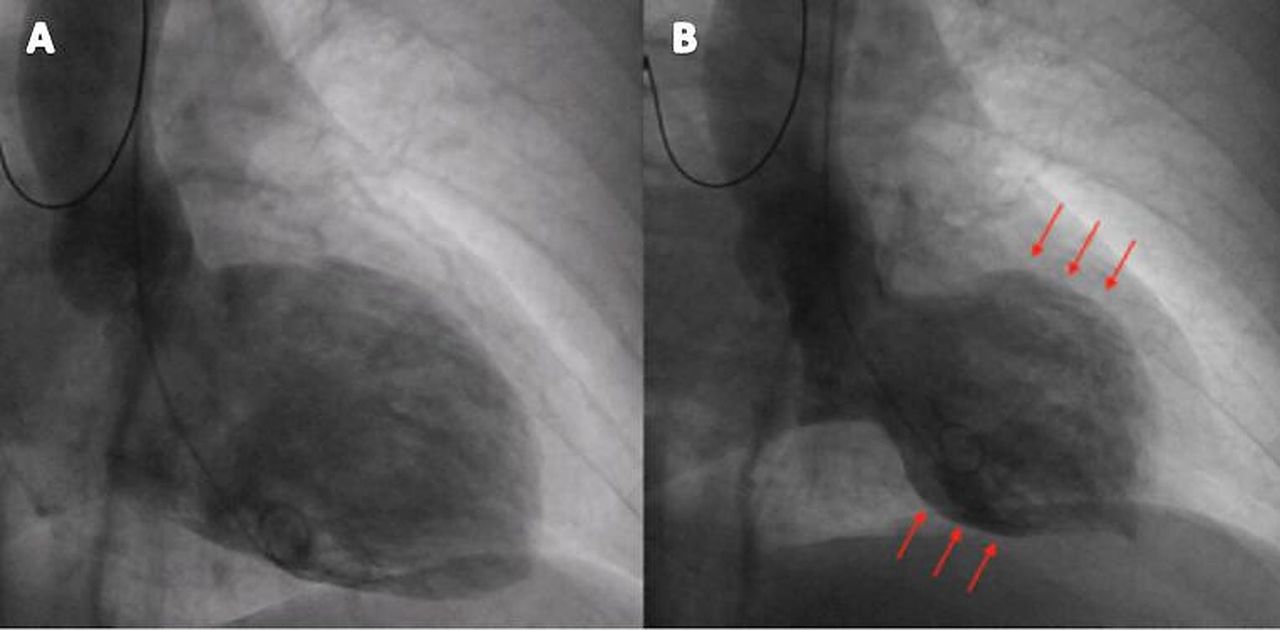
(A,B) Left ventriculogram which shows mid-ventricular wall hypokinesis with apical ballooning, as marked by the arrows in B, suggestive of Takotsubo cardiomyopathy.
Transthoracic echocardiography confirmed the findings of mid-cavity dilatation and preserved contraction of the basal and apical segments, with moderately reduced systolic function (left ventricular ejection fraction (LVEF) ~40%, Simpson’s biplane method). Cardiac MRI (CMR) performed 9 days following presentation demonstrated improvement of systolic dysfunction, with LVEF incrementing to 55% but ongoing residual mid-anterior wall segment hypokinesia with associated mid-wall late gadolinium enhancement (figure 3A,B).
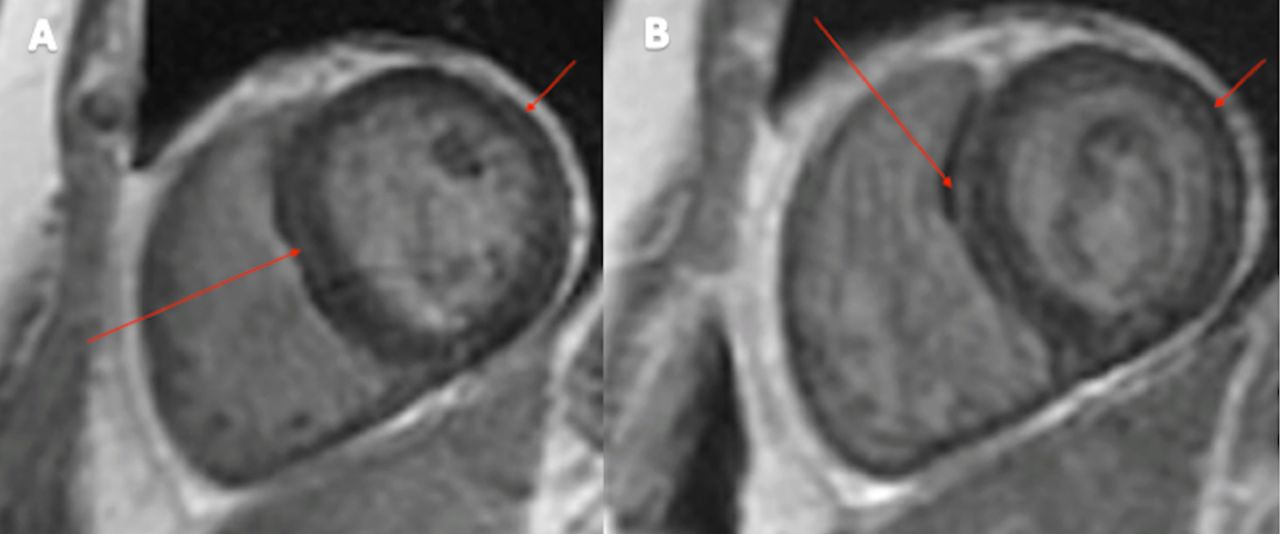
(A,B) Cardiac MRI demonstrating mid-wall late gadolinium enhancement (red arrow) indicative of mild fibrosis.
Thyroid function tests performed in the setting of persistent sinus tachycardia were consistent with thyrotoxicosis (thyroid-stimulating hormone (TSH) <0.01 mU/L, normal ~0.30–5.00 mU/L; free tetraiodothyronine (T4) >64.4 pmol, normal ~9.10–19.6 pmol/L; and free triiodothyronine (T3) >30.7 pmol/L, normal ~2.4–5.9 pmol/L). Thyroid antibodies were subsequently performed and were consistent with Graves’ disease, with elevated TSH receptor antibody of 5.5 IU/L (normal <1.9 IU/L) and normal thyroperoxidase antibodies of 0.2 IU/mL (normal ≤6 IU/mL). A clinical diagnosis of thyroid storm was made based on the Burch-Wartofsky Point Scale score of 55 points, with presence of atrial flutter (peak heart rate 170 beats per minute), vomiting and lethargy.6
Differential diagnosis
Differential diagnoses for the patient’s presentation of chest tightness with associated shortness of breath, vomiting and sinus tachycardia include cardiac, pulmonary and oesophageal aetiology (table 1). Her initial ECG demonstrated sinus tachycardia with no ischaemic changes. Her hs-cTnT was elevated and a primary diagnosis of non-ST-elevation myocardial infarction (NSTEMI) was made, with differentials including spontaneous coronary artery dissection (SCAD) and coronary artery spasm. Coronary angiography demonstrated mild coronary artery disease with no evidence of SCAD or acute plaque rupture. The left ventriculogram was suggestive of Takotsubo cardiomyopathy.
Differential diagnosis for chest pain
The D-dimer assay that was performed to investigate dyspnoea and chest tightness was elevated (0.62 mg/L, normal <0.50 mg/L). A CT pulmonary angiogram (CT-PA) was performed and found no evidence of pulmonary embolism. There was also no evidence of tension or spontaneous pneumothorax nor oesophageal perforation on CT-PA.
Echocardiography confirmed the presence of mid-cavity dilatation and anterior wall hypokinesis, consistent with the left ventriculography results, and a diagnosis of Takotsubo cardiomyopathy was made.
Treatment
Treatment was instituted for thyroid storm in the setting of Graves’ thyrotoxicosis as well as Takotsubo cardiomyopathy. The thyroid storm was initially managed with a combination of oral propylthiouracil 200 mg three times per day, intravenous hydrocortisone 100 mg four times per day, oral cholestyramine 4 g two times per day and propranolol 40 mg three times per day. Propylthiouracil was changed to carbimazole 20 mg three times per day subsequently following acute derangement in liver function tests. Intravenous hydrocortisone was ceased after 5 days following significant improvement in symptoms. Antiplatelet therapy was ceased following confirmation that Takotsubo cardiomyopathy was the cause of myocardial injury.
Guideline-based management of heart failure was instituted with commencement of perindopril, which was uptitrated to 5 mg daily on discharge and spironolactone 25 mg daily. The patient remained on propranolol on discharge for ongoing management of symptoms of hyperthyroidism.
Outcome and follow-up
Following significant symptomatic improvement after 7 days of inpatient treatment, the patient was discharged home. Her list of new medications on discharge included propranolol 30 mg three times per day, carbimazole 15 mg three times per day, further 3 days of cholestyramine 4 g two times per day, perindopril 5 mg daily and spironolactone 25 mg daily. Repeat thyroid function tests were completed 4 weeks later and showed significant improvement in thyroid function tests (T4 16.8 pmol/L, T3 8.6 pmol/L, TSH <0.01), demonstrating good response to treatment. With ongoing endocrinology outpatient follow-up, her carbimazole doses have been readjusted in accordance with her repeat thyroid function tests. A repeat transthoracic echo done 6 weeks later showed normal left ventricular systolic function and complete resolution of the regional wall motion abnormalities.
Discussion
Takotsubo cardiomyopathy, also known as broken heart syndrome or stress cardiomyopathy, was first reported in 1990 and can cause transient heart failure.7 Takotsubo cardiomyopathy is characterised by transient left ventricular regional wall motion abnormalities, as seen in our case, and they are not usually confined to a single epicardial coronary artery distribution.1 Its presentation is a mimic of ACS, with 1%–2% of ACS presentations subsequently diagnosed with Takotsubo cardiomyopathy,8 usually with a history of recent emotional or physical stress. Investigations reveal electrocardiographic abnormalities that resemble myocardial infarction and elevated troponin levels.9 However, coronary angiography demonstrates absence of occlusive coronary artery disease.9
CMR can assist in the non-invasive assessment of Takotsubo cardiomyopathy. CMR can demonstrate characteristic wall motion abnormalities as well as evidence of myocardial inflammation, which can be reversible.10 Other CMR findings include hyperenhancement of the myocardium on T2-weighted imaging, consistent with oedema, present in the area of regional wall motion abnormality.10 This characteristic finding was evident on our patient’s CMR (figure 4A,B). The presence of late gadolinium enhancement does occur in Takotsubo cardiomyopathy, although with a pattern different from myocarditis, ischaemia or infiltration, and its presence cannot be used to rule in or out Takotsubo cardiomyopathy.11

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A,B) Cardiac MRI oedema sequence demonstrating mild hyperenhancement of the left ventricle on T2 sequence suggestive of inflammation. (B) The red arrow indicates oedema in comparison with the white arrow showing normal appearance in oedema sequence.
The most common anatomical variant of Takotsubo cardiomyopathy is characterised by apical ballooning with hyperkinetic basal walls, resembling an octopus pot, and is present in up to 80% of cases. Other patterns include mid-ventricular, basal or focal.1 Our case demonstrated a mid-ventricular variant, which is present in 14.6% in the International Takotsubo Registry, with basal and focal form accounting for 2.2% and 1.5% of cases, respectively.12
Takotsubo cardiomyopathy occurs predominantly in postmenopausal women. This is attributed to increased levels of anxiety, depression, endothelial dysfunction, and increased sympathetic activity and neuropeptide Y (NPY) levels.1 Increased NPY release from presynaptic terminations may have a direct toxic effect and cause coronary vasoconstriction or microvascular dysfunction. Despite the predominance of postmenopausal women, no study has provided evidence on the association between sex hormone levels and Takotsubo cardiomyopathy.4
The pathophysiology of Takotsubo cardiomyopathy is complex, with multiple mechanisms theorised to be involved. The neuroendocrine axis is proposed to be involved, with catecholamine-mediated myocardial damage due to either direct toxicity and/or microvascular dysfunction as well as sensitisation of the myocardial tissue to sympathetic hormones by thyroid hormones exacerbating the catecholaminergic-mediated myocardial tissue damage through synergism.1 12 13 Other possible mechanisms include elevation of circulating catecholamine levels, but this continues to be a controversial theory.1 Abnormal thyroid hormone concentrations have been reported in patients with Takotsubo cardiomyopathy, but the causal association has not been fully established.2 3 Rare cases of myocarditis with Graves’ disease have been documented as well.
Thyroid hormones have similar effects to catecholamine-mediated sympathetic stimulation of beta-adrenergic receptors.14 Excess thyroid hormones, such as in Graves’ thyrotoxicosis, can lead to increased cardiac stimulation, manifesting clinically with tachyarrhythmia, inotropy and hypermetabolism.5 Thyroid hormones enhance cellular response to catecholamine action, and in thyrotoxic states lead to increased beta-adrenoreceptor density in humans, with higher physiological concentrations of adrenoceptors located at the cardiac apex.5 Other thyroid hormone effects are enhancement of beta-adrenergic cell-mediated functions and downstream elevation of cyclic AMP levels.5 Our case is unique as we observed a mid-ventricular Takotsubo rather than apical ballooning. Normal or low levels of catecholaminergic hormones have been observed in thyrotoxicosis. Therefore, synergistic enhancement of catecholaminergic action by thyroid hormone excess could explain this presentation.
Optimal management of patients with Takotsubo cardiomyopathy has not been established, with mainstay of therapy focused on management of complications.1 Heart failure therapy is often commenced with blockade of renin-angiotensin-aldosterone system and commencement of cardioselective beta-adrenergic receptor blockers in haemodynamically stable patients. Recurrent episodes of Takotsubo cardiomyopathy have been reported to occur in 2%–4% of cases.12 There is no evidence-based therapy to guide prevention of recurrence, although experts recommend long-term beta-adrenergic receptor blockade. Long-term follow-up is required as death from all-cause mortality occurred at 5.6%/patient-year, with major adverse cardiac and cerebrovascular events occurring at 9.9%/patient-year within the International Takotsubo Registry.12
Our case further highlights the importance having increased awareness among clinicians of the potential role of abnormal thyroid hormone levels in Takotsubo cardiomyopathy and to consider ordering appropriate thyroid function tests and institution of appropriate therapy.
Patient’s perspective
It was a terrifying experience but I am extremely grateful for what the doctors have done to diagnose and manage my condition.
Learning points
Patients with thyrotoxicosis can develop cardiovascular complications that include tachyarrhythmias (atrial fibrillation, atrial ectopics, etc), and Takotsubo cardiomyopathy should be increasingly noted as a potential complication.
Takotsubo cardiomyopathy is a differential diagnosis in patients presenting with symptoms consistent with acute coronary syndrome.
Following diagnosis of Takotsubo cardiomyopathy, investigation for underlying hyperthyroidism is recommended.
Treatment of Takotsubo cardiomyopathy should include treating the aetiology of the disease as well as institution of heart failure medications.
More studies are required to determine the exact pathophysiology of Takotsubo cardiomyopathy.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to acknowledge Dr Nilesh Mehta (Cardiology Consultant), who performed the angiogram as well as the left ventriculography, Professor William van Gaal (Director of Cardiology), who provided us permission to conduct this case report, and Dr Suresh Varadarajan (Endocrinology Consultant) and the rest of the endocrinology team for guiding and managing the patient’s Graves’ thyrotoxicosis.
Footnotes
Twitter @robinwjsia
Contributors RWJS is the corresponding author and is the main person responsible for carrying out this research by obtaining consent from the patient, collecting patient information, organising and obtaining results from the investigations, and subsequently writing up the case report, and holds responsibility for the integrity of this case report as well as the accuracy of any part of this work. NDS, who is a cardiology registrar, was heavily involved in the care of the patient. NDS also guided, provided advice and edited the case report. CW is a consultant cardiologist specialising in cardiac imaging who conducted the cardiac MRI and interpreted and selected optimal images for this case report. NS is a consultant cardiologist specialising in cardiac imaging who was the main supervisor of this case report and has also conducted some cardiac imaging (echocardiogram) on the patient.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.