Article Text

Abstract
We report a 4-year delay in diagnosing a combined carotid arterial and jugular venous styloid compression. The symptoms, which included dull neck pain, dizziness, intermittent diplopia, tinnitus, severe incapacitating right side headache and eye bloating, were challenging and wrongly attributed initially to various facial neuralgias. The patient presented during COVID-19 pandemic and was labelled as ‘carotidynia’ first and later as a transient perivascular inflammation of carotid artery syndrome. Combined targeted duplex ultrasonography and CT angiography with 3D reconstruction revealed a long styloid process and its tendinous-ligamentous attachments, injuring the internal carotid artery. Moreover, there was substantial internal jugular vein compression on a long C1 transverse process with a nutcracker syndrome. Release of the tendinous portion of the long styloid process and repair of the carotid artery pseudoaneurysm ended the patient’s complaints and allowed him to have a better quality of life.
- Vascular surgery
- Otolaryngology / ENT
- Head and neck surgery
- Medical management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Eagle syndrome is a rare syndrome attributed to the styloid process’s elongation and associated mineralisation or ossification of the stylohyoid ligament.1–3 The symptoms are challenging and, at times, wrongly attributed to various facial neuralgias. There are two distinct types of primary Eagle syndrome: primary stylo-carotid and stylo-jugular syndrome. The former refers to stenosis or internal carotid artery (ICA) dissection, and the latter is due to impingement on the internal jugular vein (IJV) with venous reflux obstruction.1–6 The secondary or classic syndrome mainly occurs post-tonsillectomy with the irritation of the glossopharyngeal nerve by an inflamed styloid process.4
We report a challenging case of combined carotid arterial and jugular venous styloid compression due to the tendinous and ligamentous attachments of the long styloid process injuring the ICA and causing a pseudoaneurysm. Concomitant, IJV compression due to a long C1 transverse process caused a venous compression by the styloid process on IJV. The patient had various complaints over 10 years, but it was exacerbated over the past 4 years. The task of diagnosing such a complex pathology requires a high index of suspicion.
Case presentation
A man in his 70s presented to his general practitioner with slowly progressive intermittent dull pain in the anterior triangle of the upper right neck for 10 years. It was associated with dizziness, intermittent diplopia, sharp agonising incapacitating right-sided headache, tinnitus and eye bloating that exacerbated over the past 4 years. The pain was localised to the tonsillar fossa and accompanied by dysphagia, foreign body sensation, sore throat and voice changes. It was worsened by head movements such as looking up and turning the face to the left side or lying on a pillow.
The patient went through several consultations over this period, including otolaryngology, neurology, neurosurgery, psychiatry and dentistry visits. The patient was a non-drinker and non-smoker, and he did not have a family history of cardiovascular disease or aneurysms. There was no history of trauma. The patient had appendectomy at the age of 14 and tonsillectomy at 32. He had transurethral resection of the prostate followed by radiotherapy in 2013 for prostatic cancer. He had a first-degree heart block with a normal coronary angiogram. His medications included statin and calcium channel blockers. Frequent MRIs of the brain performed before he presented to us delineated mild chronic microvascular ischaemic changes, which were age-appropriate, but no acute intracranial events. The MRIs were confined to the brain, and he did not have an MRI of the cervical region or an Magnetic Resonance Angiography (MRA) of the carotid arteries.
The patient was admitted to a regional hospital during the COVID-19 crisis and was diagnosed as having carotidynia. Later on, the physician managing the patient diagnosed him as having a transient perivascular inflammation of carotid artery syndrome, attributing the complaints to a post-COVID subclinical infection. Despite normal C reactive protein, erythrocyte sedimentation rate and white blood cell count, he was started on a short course of prednisolone for 4 weeks with dual antiplatelet therapy and was referred to our practice after that.
Investigations
A targeted duplex ultrasound demonstrated a saccular right ICA pseudoaneurysm. A CT-carotid angiogram and the subsequent 3D reconstruction showed a 3.2 cm long styloid process and a long transverse cervical process at C1 (figure 1). The styloid process extended to the ICA, which was highly tortuous, and there was a visible indentation on the ICA. The indentation corresponded to the area of the perivascular sympathetic plexus around the ICA. The irritation of the sympathetic plexus explained the constellation of symptoms, that is, Horner syndrome and related dizziness with neck pain.

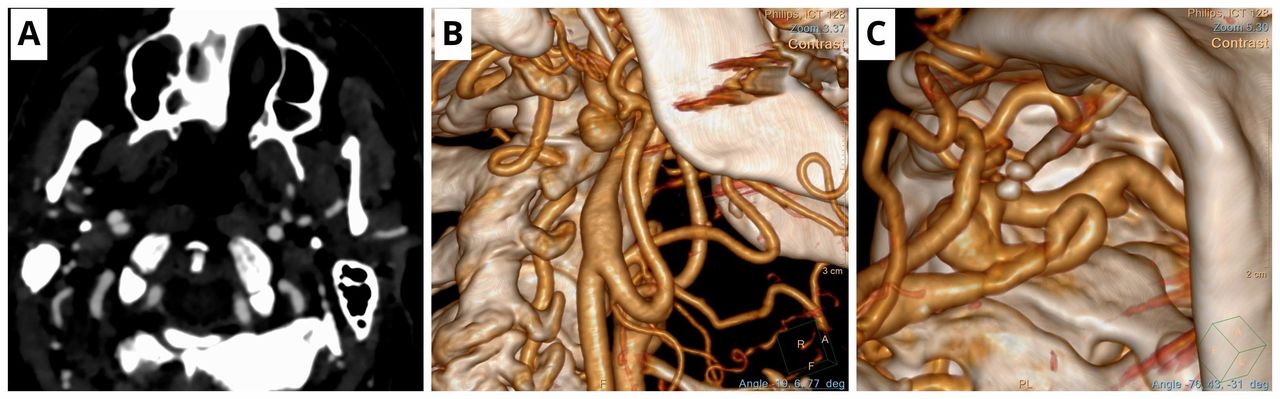
(A) A CT angiography axial view depicting right internal carotid artery (ICA) pseudoaneurysm and compression of right internal jugular vein between the styloid process and long C1 transverse process. (B) A 3D reconstruction (lateral view) showing 32 mm long right styloid process strapping the two loops of the right ICA with the formation of a pseudoaneurysm of mid-ICA. Notice the elongated C1 transverse process just behind the ICA pseudoaneurysm. (C) A 3D reconstruction (caudal view) showing a 32 mm long right styloid process strapping the two loops of the right ICA with the formation of a pseudoaneurysm of mid-ICA. The mineralised ossified styloid ligament is strapping the looped ICA. Notice the proximity of the ligamentous, tendinous part of the right styloid process.
Concomitantly, the long C1 transverse process was compressing the right IJV against the styloid process, which explained the incapacitating headaches, tinnitus and eye congestion.
Differential diagnosis
The symptoms related to Eagle syndrome can be confused with a wide variety of facial, dental and temporomandibular diseases, including facial neuralgias like trigeminal neuralgia, glossopharyngeal neuralgia, temporal arteritis, hyoid bursitis, migraine-type headaches, cervical arthritis, temporal arteritis, carotid artery dissection, salivary gland diseases, head and neck tumours, oesophageal diverticula, otitis media, faulty dental prostheses and cervical arthritis.1 The elongated styloid process instigates continuous irritation of the cranial nerves, most commonly the glossopharyngeal nerve, with subsequent throat and neck pain. Glossopharyngeal neuralgia is typically more dull and constant. Similarly, ageing could be associated with degenerative and inflammatory changes in the tendinous portion of the stylohyoid insertion, a condition called ‘insertion tendinosis’ that causes pain in the distribution of glossopharyngeal nerve resembling an Eagle syndrome and referred to as pseudostylohyoid syndrome.1 7 8
Treatment
Surgery is the definitive treatment that includes styloidectomy and/or release of the tendinous stylohyoid insertion. An open cervical neck approach was adopted for our patient. Following a cervical neck incision along the sternocleidomastoid muscle’s anterior border, the styloid process’s distal end was lifted, and its proximity to the hypoglossal, glossopharyngeal, vagus and chorda tympani of the facial nerve was observed. The ligamentous and/or tendinous structure strapped to the proximal ICA was cut. The styloid process’s pointing and angle had sprung away to enlarge the space for both the artery and the vein (figure 2). Once the styloid process recoiled out of the surgical field, the whole space was freed to perform an end-to-end ICA anastomosis (figure 3). The IJV expanded, and its physiological response was restored with the visualisation of the ‘A’ wave and oscillation.

Intraoperative image: (A) Reconstruction with the two loops of the right internal carotid artery (ICA) with the internal carotid pseudoaneurysm, notice the close relation of the long styloid process to the neurovascular structures. Of importance is the total collapse of the right internal jugular vein. (B) Excision of the ossified styloid process, repair of right ICA pseudoaneurysm with end-to-end anastomosis. Notice that the styloid process had sprung out of the field after cutting its tendon. The jugular vein starts to refill typically with the bluish discolouration.
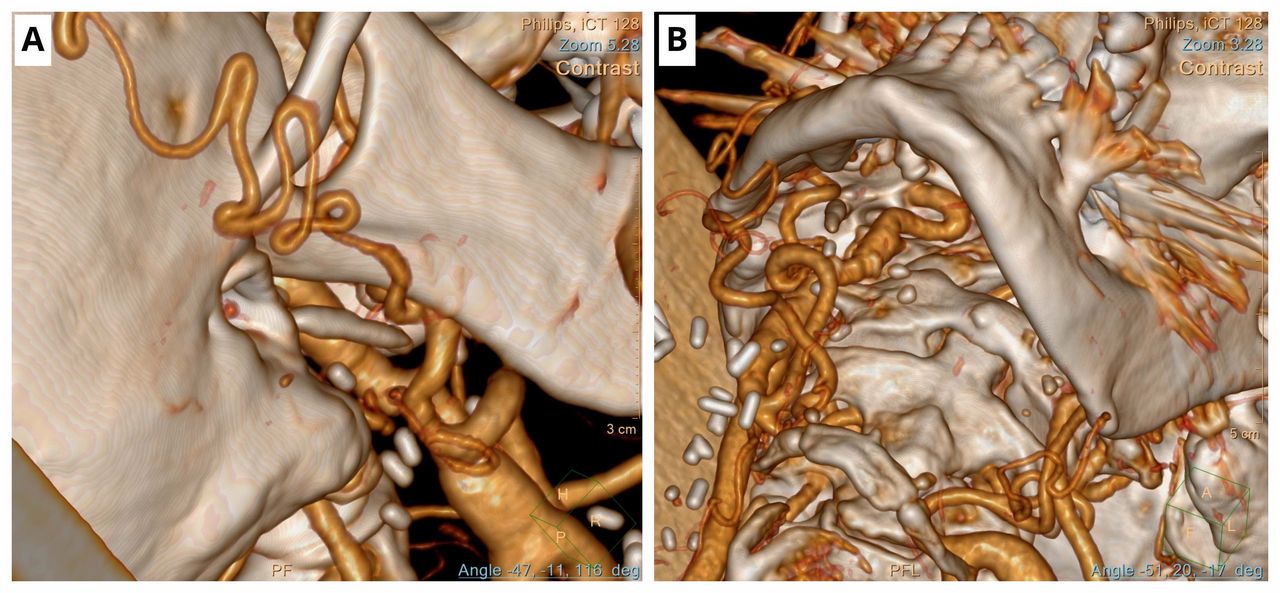
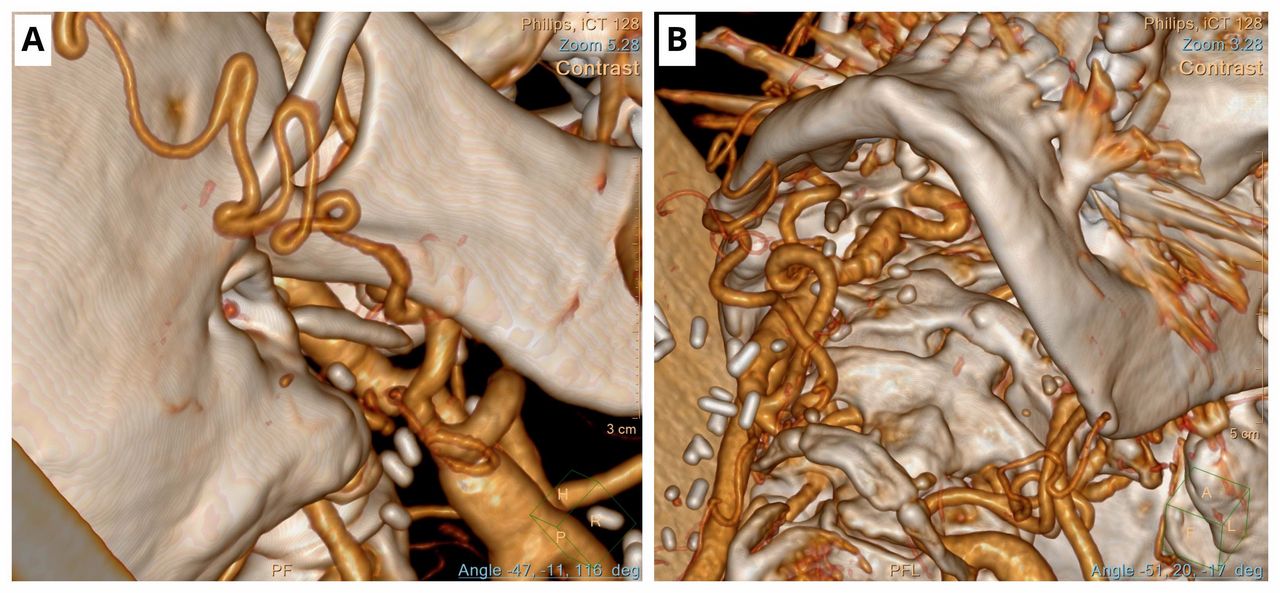
A 3D reconstruction: (A) Post open surgical repair of right internal carotid artery (ICA) aneurysm with end-to-end anastomosis and excision of the ligamentous-tendinous part of the styloid process. The styloid process’s pointing and angle had sprung away to enlarge the space for both the artery and the vein. (B) Post open surgical repair of right ICA aneurysm with end-to-end anastomosis and excision of the ligamentous-tendinous part of the styloid process. The styloid process’s pointing and angle had sprung away to enlarge the space for both the artery and the vein. The ICA is far away from the C1 transverse process.
The ligamentous distal part of the styloid process was in close contact with the ICA, which predisposed the pseudoaneurysm and minimised the space for IJV capacitance due to the nutcracker (figure 4).

Comparative preoperative and postoperative CT angiography: (A) Preoperative coronal view depicting the right internal jugular vein compression between the styloid and long C1 transverse processes. Notice the volumic space difference between the right and left side with the normal left side is as twice as the right side. (B) Postoperative coronal view after releasing the ligamentous-tendinous ossified distal styloid process. The right volume had increased 50% from its preoperative size compared with the normal left side.
Outcome and follow-up
After the surgery, the patient had a complete resolution of the neck pain, dizziness, tinnitus and diplopia, and returned to normal activities. A postoperative duplex scan and CT angiogram showed the IJV had expanded in volume, and the right ICA was straight and patent.
Discussion
The carotid artery and jugular vein compression by anomalous cervical structures is scarce, and the development of neurovascular complications related to mechanical impingement is an exception.4 6 In 1937, ‘Eagle syndrome’ or ‘stylocarotid artery syndrome’ was reported.2 In his first report, Dr Watt Eagle postulated that Eagle syndrome occurs following surgical trauma post-tonsillectomy and local chronic inflammation results in osteitis, periostitis or tendonitis of the styloid process and stylohyoid ligaments. This, in turn, results in reactive, ossified hyperplasia of the ligament.1 6–8 Reactive hyperplasia and reactive metaplasia result in the overgrowth of the styloid process with subsequent ossification. Scar tissue around the styloid’s apex post-tonsillectomy can compress or strain the neurovascular structures in the retrostyloid compartment with abnormal angulation of lengthy styloid process. The abnormal styloid process can irritate the adjacent musculature or mucosa with fibrosis involving the 5th, 7th, 9th and 10th cranial nerves.
The normal styloid process is 2.5 cm in length, and any process longer than 2.5 cm is considered abnormal elongation. A long styloid process is incidental in about 4% of the general population, and only 4% present with symptoms attributable to elongation of the styloid. Patients are on average older than 30 years of age at the time of presentation, with a female-to-male predominance of 3:1.1 7
The stylohyoid complex, encompassing the styloid process, the stylohyoid ligament and hyoid bone, is in the vicinity of ICA and IJV.4 6 Neurological symptoms triggered by compression of the extracranial ICA or IJV due to an elongation of the styloid process by more than 30 mm caused by ossification of the stylohyoid ligament.1 4–7 In this case, the elongated styloid process combined with an extended cervical transverse process at C1 caused venous compression. It is likely that the venous compression exacerbated an inflammatory process, leading to the proliferation of stylohyoid ligament’s ossification. Then as thickness and length of the styloid process increased, it impinged on the internal carotid with irritation of the arterial sympathetic fibres causing diplopia.
Eagle syndrome usually presents with a characteristic dull and throbbing pain from the elongated styloid process, aggravated with deglutition and objectively reproduced by palpating the tonsillar fossa. In addition, the anomalous stylohyoid complex anatomy can provoke ICA-IJV injury, such as dissection or thrombosis, with neck rotation, stretching, talking, laughing and swallowing.6–10 Intraoral palpation can identify an elongated styloid process by placing the index finger in the tonsillar fossa and applying gentle pressure. These manoeuvres can reproduce the pain, or the patient can feel it referred to the ear, face or head. A standard styloid process length is usually impalpable.
A CT is the most accurate diagnostic test.1 6 7 However, CT angiogram lacks dynamic information. Therefore, a 3D CT reconstruction of the neck enables precise measurement of the length of the styloid process and the ossified stylohyoid ligament. Positional changes during CT angiogram can uncover the pathological anatomical relationship between carotid arteries and IJV with the cervical bony and cartilaginous structures, particularly during head rotation and swallowing. Orthopantomogram and CT can both be used to assess the styloid process/stylohyoid ligament complex. CT with contrast medium and 3D reconstruction allows correct measurement of the length and angulation of the styloid process and evaluation of its relationships with the vascular and lateral-cervical nerve structures and should be obtained with the patient’s head appropriately positioned to reproduce symptoms that may demonstrate mechanical stenosis of the ICA or IJV.
Management is surgical, and cervical neck surgery with styloidectomy is the definitive treatment.1 11–13 However, ligamentous ossification of the stylohyoid process can lead to chronic impingement of the surrounding neurovascular structures, resulting in various complications, including dissection and/or pseudoaneurysm, which can complicate the management process.14 15 ICA or IJV compression by the styloid process can cause transient ischaemic attacks, sympathetic nerve irritation, severe bouts of headache or perimesencephalic subarachnoid haemorrhage.16 17 ICA proximity to the styloid or hyoid bone is a definite risk factor for carotid dissection or pseudoaneurysm formation even if the processes length is average due to ligamentous or tendinous ossification of the styloid ligament.14 15
EXTracranial INternal Carotid arTery pseudoaneurysms (EXTINCT)
EXTINCT accounts for 1% of arterial aneurysms.18 19 Any segment of the common carotid artery, external carotid artery and ICA can be affected, although the ICA is most commonly involved.19 The pathological presentations of the stylohyoid complex include carotid dissection, pseudoaneurysm, stenosis or occlusion due to direct compression, and pressure-induced plaque formation and rupture due to constructional changes at the carotid wall leading to alterations in blood flow and shear force. This repetitive mechanical interference on the carotid artery wall can cause a vessel wall injury and intimal thrombus formation with cerebral embolisation, that is, triggered recurrent neurovascular events.20
In a multicentre case-control study of carotid artery dissection patients, Renard et al9 demonstrated that shorter distances between the stylohyoid complex and ICA result in mechanical injury and predispose to carotid artery dissection. Schneider et al15 considered the phenomenon of mechanical trauma to the ICA leading to thrombus formation, embolisation and recurrent TIAs, and called it carotid artery entrapment syndrome.
There are no guidelines or treatment algorithms due to the scarcity of cases. The rarity of extracranial primary internal carotid pseudoaneurysms associated with Eagle syndrome means that there is a lack of evidence and publication bias in selecting treatment options. However, surgical partial bone resection and the release of ligamentous-tendinous entrapment have proved to be safe and effective, helping to restore patients’ freedom of neck movement and consequently improve physical and psychological quality of life.11 21
When embolisation is suspected, or in cases of ICA dissection, anticoagulation therapy in the early phase is considered in the absence of contraindications.20 Currently, the challenges in managing such patients depend on the suitability of endovascular stents to the target area, length of vessel injury and vessel angulations.21 22 Repair of EXTINCT is mandated in almost all cases, as the risk of fatal complications related to embolisation, rupture and local compression is high.13 23 The adoption of conservative management had been linked to 71% mortality, and catastrophic consequences have been reported if the ICS pseudoaneurysm is ligated.24
We concur with Bartoli et al25 that saccular aneurysms of the extracranial ICA are rare and represent <1% of all revascularisation for the ICA. Our case is an Attigah et al11 type I aneurysm that required an end-to-end repair due to severe ICA angulation, and two S-shaped loops precluded any endovascular intervention. Therefore, contrary to the recommendations by Angiletta et al,21 endovascular therapy was not feasible.22
Eagle jugular syndrome
Eagle jugular syndrome is a variant of Eagle syndrome. An elongated styloid process adjacent to the transverse process of C1 causes the compression of the IJV, leading to intracranial hypertension and cerebral haemorrhage.26 27 The literature has scrutinised the heterogeneity of the Eagle clinical picture. Zamboni et al17 documented that styloid process elongation can have variable consequences, and it can cause impingement on any anatomical structures. Significant differences clinically delineate this jugular variant compared with the classic and carotid variants. Headache and perimesencephalic haemorrhage are more prominent symptoms with IJV compression.
For both the ICA dissection and IJV nutcracker syndromes, the styloid process length is the primary causal factor.1 7 28 The uniqueness in our patient is the combination of arterial Eagle syndrome with venous nutcracker internal jugular syndrome due to the concomitant elongated transverse process of the right C1 (figure 5).

Schematic diagram depicting primary styloid-carotid-jugular syndrome: (A) Venous nutcracker internal jugular syndrome is due to compression of the internal jugular vein (IJV) between the elongated transverse process of the right C1 and proper styloid process and its ossified mineralised ligamentous-tendinous attachments. (B) The long right styloid process strapping the two loops of the right ICA with the formation of a pseudoaneurysm of mid-ICA. The mineralised ossified styloid ligament is strapping the looped ICA. Notice the proximity of the ligamentous-tendinous part of the right styloid process to the pseudoaneurysm. (C) Combined carotid arterial and jugular venous styloid compression due to the tendinous-ligamentous of the long styloid process injuring the ICA causing a pseudoaneurysm, with IJV compression due to a long C1 transverse process that caused a nutcracker with the styloid process on IJV. The elongated styloid process instigates continuous prickliness of cranial nerves, most commonly the glossopharyngeal nerve, hypoglossal nerve, trigeminal, facial and vagus cranial nerves. (Authors declare that these figures are original and drawn by them.)
The imprecise symptoms portrayed by IJV compression syndrome often result in delayed or missed diagnosis29 30:
Head symptoms: Severe bouts of unilateral headache, head noise, dizziness and memory decline.
Eye symptoms: Eye congestion, diplopia, blurred vision and visual field defects.
Ear symptoms: Tinnitus, high-frequency hearing decline, neck discomfort or sleeping disorder.
The IJV J3 segment is most frequently involved.5 31 The jugular venous wall is thinner and lacks smooth muscle and elastic fibres. IJV is helpless under extrinsic compression, which is why cervical bony cartilaginous structures deform IJV.7 32 A targeted duplex ultrasound scan of the IJV is the most sensitive,6 but magnetic resonance venography is superior to computed tomographic venography for accuracy of diagnosis.28 Li et al4 documented that after an accurate diagnosis of Eagle jugular syndrome, conservative treatments are worthless for the styloid-induced IJV syndrome, and jugular stenting offers no benefit. Styloidectomy is the only effectual management.7 9 26
Styloidogenic jugular compression is a nosological entity, having a variety of syndromic names, including ‘styloidogenic-cervical spondylotic internal jugular venous compression’, ‘Eagle jugular syndrome’ or ‘styloid-induced IJV stenosis’.4–6 31 Venous flow impairment due to the styloidogenic compression can result in an imbalance in venous-cerebrospinal fluid and the lymphatic system. The symptomatologies of headache, tinnitus, insomnia and visual impairment are almost pathognomonic.17 29–31 33 These constellations of symptoms are not explained by any other common neurosurgical or ear, nose and throat disorder.
Current literature does not concede to any robust conclusion but recommends the necessity to collect more clinical data. Failure of conservative treatment commands a surgical or endovascular approach and must be tailored to each case individually to achieve favourable results and reduce possible complications.6
Combined carotid-jugular Eagle syndrome
We believe that this challenging, complex case of nutcracker jugular vein compression and ICA pseudoaneurysm due to the ossification of the stylohyoid ligamentous-tendinous process and C1 transverse process elongation is one of the first reported cases. The traditional Eagle syndrome focuses on arterial compression and does not include the combined arterial and venous compression syndrome. Therefore, we propose a classification of the primary stylo-carotid and stylo-jugular syndrome (figure 6):
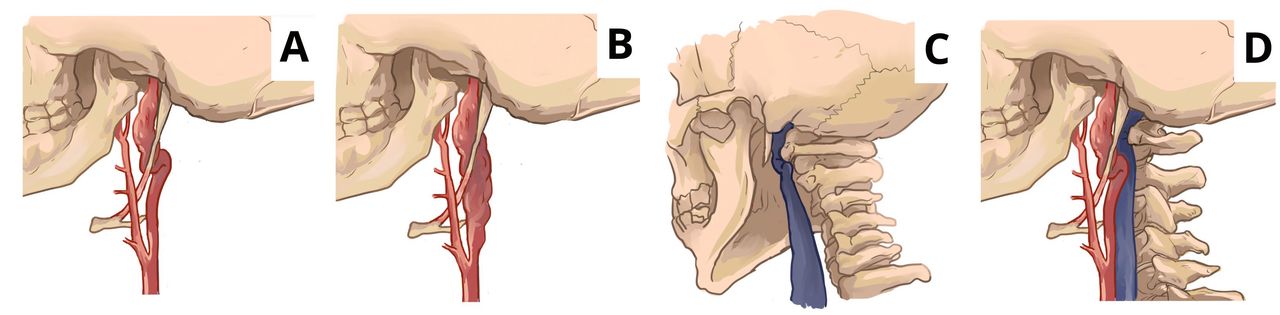
Classification of primary Eagle syndrome: (A) Type IA: Primary stylo-carotid syndrome with mid-internal carotid artery (ICA) involvement. (B) Type IB: Primary stylo-carotid syndrome with proximal and mid-ICA involvement. (C) Type II: Primary stylo-jugular syndrome with impingement on the internal jugular vein. (D) Type III: Combined primary stylo-carotid-jugular syndrome. (Authors declare that these figures are original and drawn by them.)
Type IA: Primary stylo-carotid syndrome with involvement of mid-ICA.
Type IB: Primary stylo-carotid syndrome with involvement of proximal and mid-ICA.
Type II: Primary stylo-jugular syndrome with impingement of the IJV.
Type III: Combined primary stylo-carotid-jugular syndrome.
The clinical presentation of our patient was the culmination of a complex symptoms resulting from both arterial and venous pathologies, which were managed accordingly (figure 7). Misdiagnoses and delayed time to diagnosis in primary stylo-carotid-jugular syndrome is due to the challenging nature of symptoms and signs.7 34 Modern diagnostic techniques tools should be employed to expedite the diagnosis of these complex syndromes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic diagram depicting: (A) Prerepair and postrepair of the primary stylo-carotid syndrome with mid-internal carotid artery (ICA) involvement. (B) Prerepair and postrepair of the primary stylo-carotid syndrome with proximal and mid-ICA involvement. (C) Prerepair and postrepair of the combined primary stylo-carotid-jugular syndrome. (Authors declare that these figures are original and drawn by them.)
Learning points
The primary stylo-carotid-jugular syndrome involves irritation of cranial nerves V-X, proximal to the mid-internal carotid artery and the J3-segment of the internal jugular vein.
Tinnitus, otalgia, pharyngeal pain, dysphagia, unilateral headache, diplopia, dizziness, foreign body sensation, pain on extending tongue, change in voice and hypersalivation sensation are hallmarks of this complex syndrome.
Targeted duplex ultrasonography with 3D reconstruciton of CT angiography is useful to elucidate the anatomical relationships and enables the exclusion of other compression syndromes.
Styloidectomy and/or styloid ligamentous-tendinous release effectively eradicates the contributing factor.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors The authors confirm contribution to the paper as follows: study conception and design: SS, YA, OS, NH; data collection: SS, YA, OS, NH; analysis and interpretation of results: NA; draft manuscript preparation: SS, YA, OS, NH. All authors reviewed the results and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.