Article Text

Statistics from Altmetric.com
Description
Implantation of intraocular lens (IOL) in eyes with weak capsular support or zonular support presents unique surgical challenges.1 Most of the published literature on scleral fixated lens (SFIOL) implantation describes techniques for the implantation of rigid 3-piece IOLs. Only a few techniques (Takkar et al2 Can3 Yamane et al4 Francesco Barca et al5 Kumar and Agarwal6) have been described until in the literature for implantation of foldable SFIOLs as mentioned in table 1. However, all these techniques require intraocular manipulation of the haptics using the handshake technique, which has a learning curve.7 We now, discuss the steps of foldable SFIOL implantation using an adaptation of the extraocular needle-guided haptic insertion technique (XNIT) that was originally described for rigid SFIOL implantation.8 In addition, we also describe a small modification in the original XNIT technique that provides an added advantage of negating the risk of intraoperative haptic rebound into vitreous cavity. This modified technique can be easily learnt and applied by the novice surgeons as well as the cataract surgeons for performing SFIOL implantation.9
Summary of ma published foldable SFIOL techniques
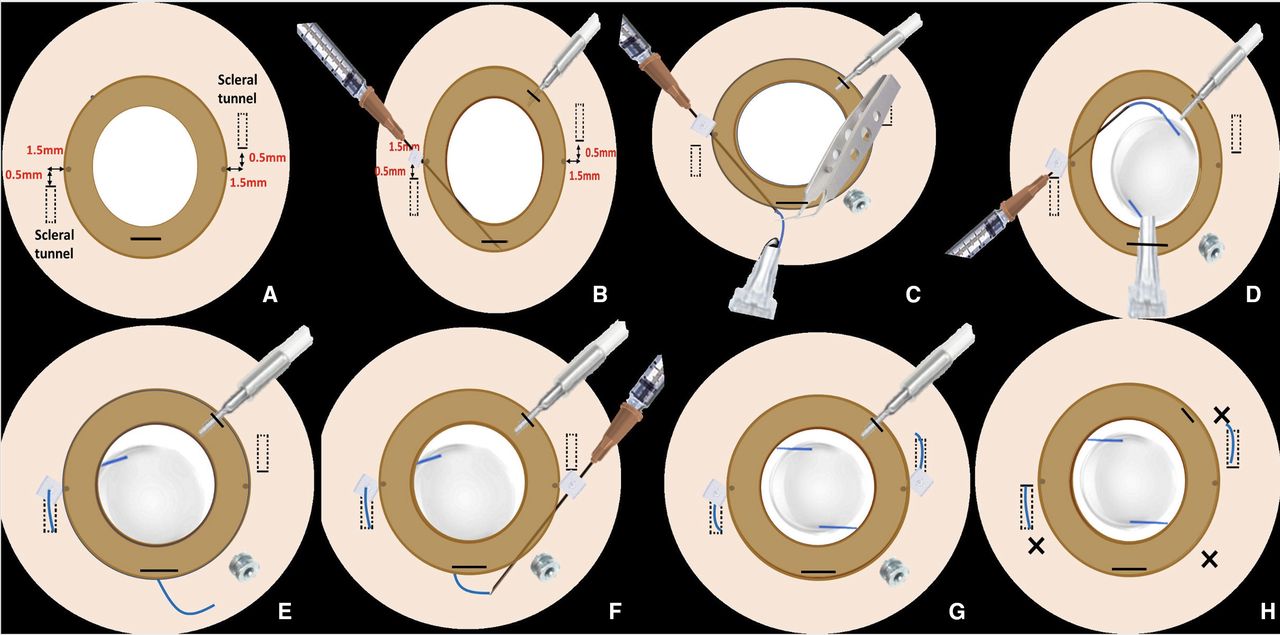
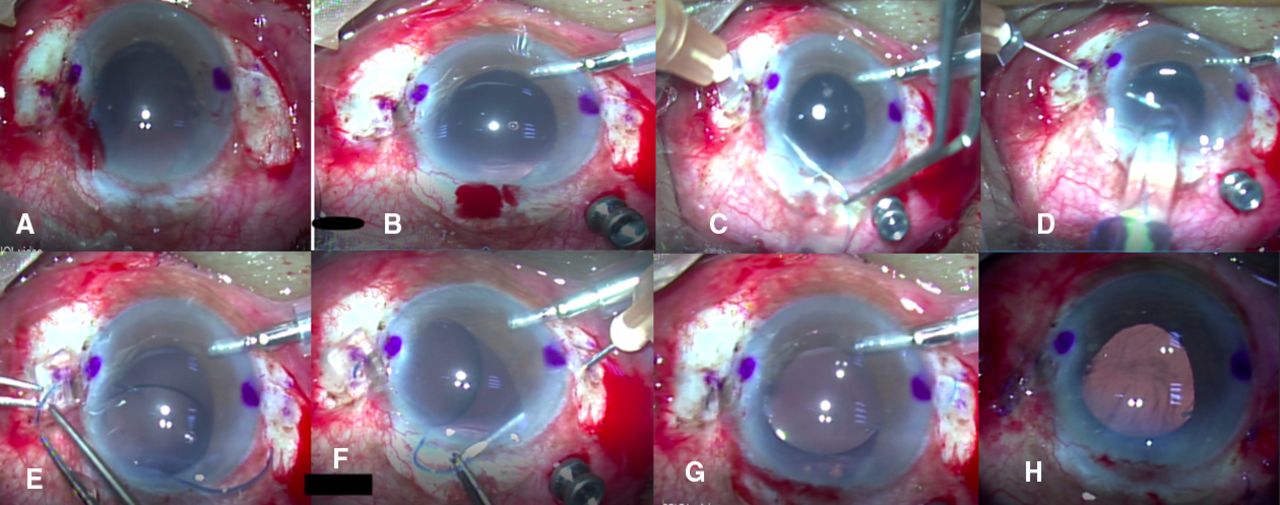
Surgical technique: Under peribulbar anaesthesia, two markings are made at the limbus 180° apart (3 and 9 o’clock positions). Limited peritomy is then done adjacent to the limbal markings (figures 1A and 2A). Two partial thickness 3 mm long scleral tunnels (one on each side) are then fashioned. Each tunnel commences 0.5 mm farther away (modification from the original XNIT technique) from the future site of sclerotomy (figures 1A and 2A). An anterior chamber (AC) maintainer is then secured (figures 1B and 2B). Limited anterior vitrectomy is then performed either through a paracentesis entry or through a single 23 pars plana port. We have used a pars plana port in the representative video (video 1). All vitreous strands in the AC, pupillary area or below the iris are excised. A 3 mm wide corneal section is then constructed superiorly spanning 12 0’ clock (figures 1B and 2B). Two half-inch-long 26 gauge (G) needles are used for haptic loading, IOL insertion and haptic exteriorisation. One needle is passed through a 2×2 mm silicone stopper made from a 240 encircling silicone band similar to the XNIT technique. The needle is then bent 1 mm from the hub and inserted into the ciliary sulcus 1.5 mm behind the limbal marking and 0.5 mm farther from the point of commencement of the scleral tunnel (figures 1A and 2A). The needle is then brought out through the corneal tunnel with the posterior lip of the wound depressed with a McPherson forceps (figures 1C and 2C). The preloaded foldable 3-piece IOL (Aurovue Multi-piece preloaded IOL, Model No: HP3600P) (no financial interests, any other 3-piece foldable IOL can be used as well) is then inserted using the needle as guide for the haptic (figure 1C). Around 3 mm of the leading haptic is injected out of the cartridge by the injector in the extraocular space. The leading haptic is then loaded into the lumen of the 26 G needle that had already been exteriorised through the corneal section. An assistant can help in guiding the leading haptic into the lumen of the needle with a McPherson forceps to ensure snug fitting and prevent subsequent slippage of the haptic. The cartridge tip is then inserted gradually through the corneal section while the needle (with the leading haptic embedded in its lumen) is simultaneously withdrawn back into the AC in a co-ordinated fashion (figures 1D and 2D). As the injector is slowly pushed, the IOL gradually unfolds in the AC. Care should be taken to push the injector only until the optic is released inside the AC. The trailing haptic should not be injected inside the AC and should be still lodged in the cartridge. The needle and the leading haptic are then slowly exteriorised through the sclerotomy site (figures 1E and 2E). The injector is then gradually withdrawn out through the corneal section and the trailing haptic is released in the extraocular space. The exteriorisation of the needle through the sclerotomy site and withdrawal of the injector from the AC should also be co-ordinated. Once the needle with the leading haptic is exteriorised, the silicone stopper is guided over the leading haptic and the needle removed (figures 1E and 2E). The stopper prevents slippage of the leading haptic inside the vitreous cavity during manipulation of the trailing haptic. The second 26-gauge needle is bent and inserted through the opposite side sclera 1.5 mm behind the second limbal marking. The trailing haptic is threaded into the needle using McPhersons forceps, exteriorised and tucked into the preformed scleral tunnel (figures 1F and 2F). The silicone stopper is removed and the leading haptic is also tucked into the scleral tunnel (figures 1G and 2G). IOL centration is ensured by adjusting the haptics. Pars plana port and peritomies are then closed (figures 1H and 2H). AC maintainer is removed and the corneal wounds are hydrated to prevent wound leakage and subsequent hypotony. We have described the outcomes of 11 cases operated using this technique in table 2.

(A)Two conjunctival peritomies are created at 3 o’clock and 9 o’clock positions, (B) AC maintainer is started and corneal incision is made, (C) the leading haptic of the 3-piece IOL is tucked into the lumen of the 26 gauge needle, (D) the IOL is slowly injected into AC, (E) the leading haptic is exteriorised and the silicone stopper is guided over it, (F) the trailing haptic is tucked into the 26 G needle, (G) the trailing haptic is exteriorised and both the haptics are tucked into the previously created scleral tunnels, (H) pars plana port and the peritomies are sutured. AC, anterior chamber; IOL, intraocular lens.
{kind=link}
{kind=link}
Animated figure showing the steps of three piece foldable SFIOL using an adaptation of the extraocular needle-guided haptic insertion technique. SFIOL, scleral fixated lens.
Patient characteristics
Large incisions may predispose to intraoperative or postoperative hypotony, choroidal detachment, postoperative astigmatism, delayed postoperative recovery, etc.10–13 Foldable IOLs eliminate the need for larger incisions for IOL insertion, thereby, reducing the postoperative astigmatism, hypotony and allows earlier visual rehabilitation.14 Also smaller incision ensures AC formed during the procedure and reduces endothelial cell injury. All the previously described techniques need intraocular manipulation of the IOL haptic which increases the risk of haptic breakage, haptic kinking, IOL drop into the vitreous cavity.15 Moreover, intraocular manipulation has a learning curve and often a hurdle for the novice surgeons. We have adapted the XNIT technique for haptic manipulation in the extraocular space which helps to overcome the problems associated with intraocular handling of the haptics. Our technique of foldable SFIOL implantation provides a simple, economic and effective option for aphakia management to the beginners as well as the experienced surgeons. It has definite advantages over previously described techniques in terms of haptic management and reduction of intraoperative complications. However, the steps of leading haptic loading, injection of IOL in the AC and exteriorisation of the leading haptic should be done carefully. Future longitudinal and comparative studies with similar techniques are needed to determine the long-term structural and functional outcomes and complications.
Learning points
Foldable scleral fixated intraocular lens implantation techniques can help to prevent complications like hypotony, choroidal detachment, astigmatism, delayed postoperative recovery.
Intraocular manipulation has a learning curve and often a hurdle for the novice surgeons.
Foldable scleral fixated lens using extraocular needle-guided haptic insertion technique can be a boon for the anterior segment surgeon which can be reproduced very easily.
Ethics statements
Patient consent for publication
Footnotes
Contributors AKD: design and performed the surgery, SS: manuscript writing, KN: manuscript review, JP: patient care.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.