Article Text

Statistics from Altmetric.com
Description
Postoperative pseudomeningoceles are characterised by extradural accumulation of cerebrospinal fluid (CSF) leaked from a surgical wound into the subcutaneous space.1 Giant cranial pseudomeningoceles are extremely rare. Herein, we describe a case of focal seizures and haemiparesis caused by decompression of a giant cranial pseudomeningocele.
An otherwise healthy man in his 40s presented with generalised tonic-clonic seizures. Imaging demonstrated a 4.7×4.0×3.6 cm extra-axial right parasagittal lesion suggestive of a meningioma (figure 1A). His seizures were controlled with antiepileptic drugs and he underwent a right parietal craniotomy for resection of meningioma. The procedure was uneventful. Postoperatively, he developed a persistent large pseudomeningocele, with no features of hydrocephalus. We managed the pseudomeningocele conservatively, expecting it would settle with time. Histopathology confirmed a WHO grade 1 meningioma.
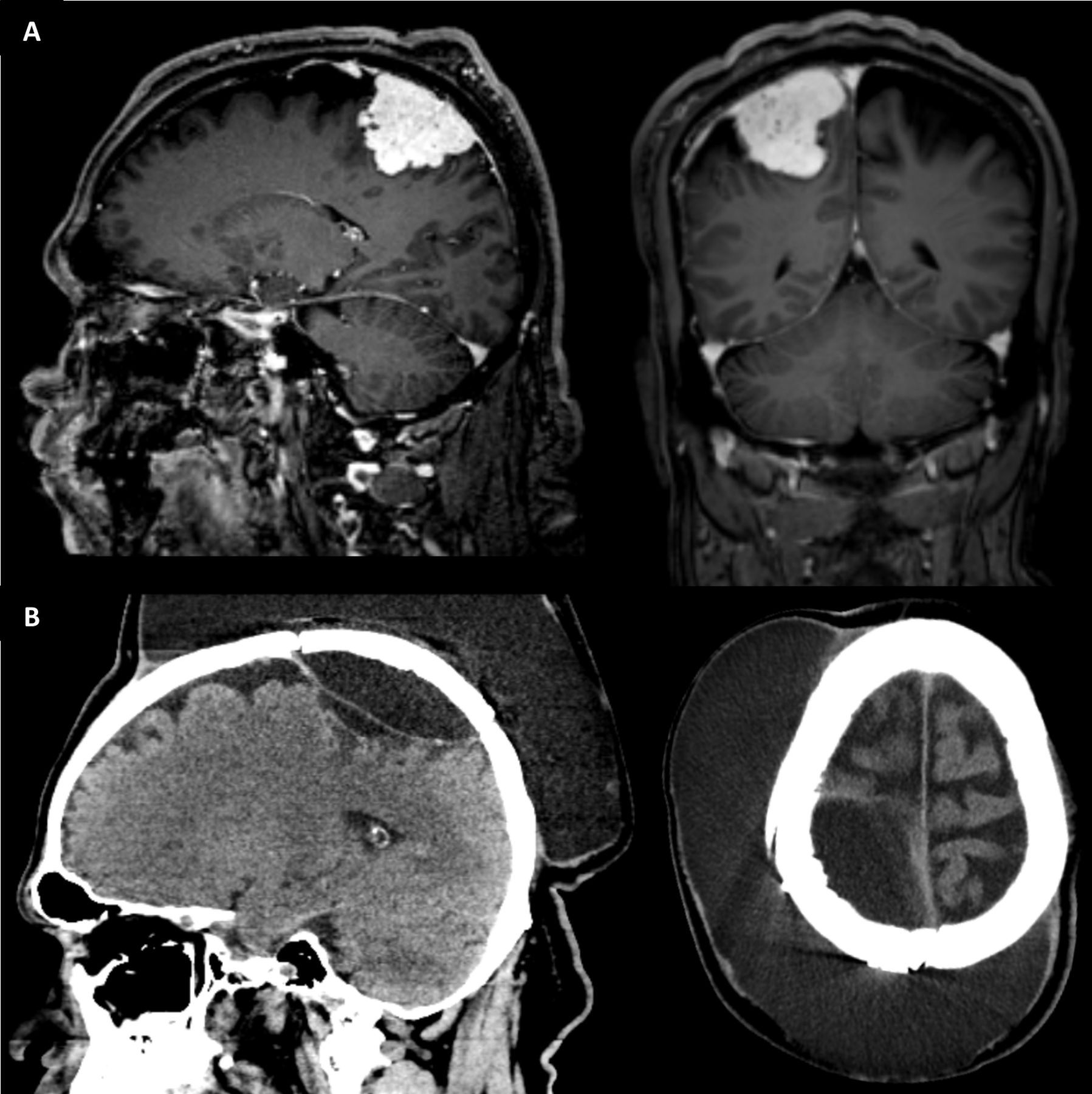
(A) Preoperative sagittal and coronal T1-weighted MRI images with gadolinium demonstrating a right parasagittal durally based tumour. (B) Postoperative CT confirmed the presence of a very large pseudomeningocele with extracranial and intracranial components.
He represented 3 months following his operation reporting problem of headache and a recent progressive increase in the size of the pseudomeningocele. On examination of the wound site, there was a very large fluctuant collection (>20 cm). He was neurologically intact. CT imaging of the brain confirmed the presence of a large subcutaneous CSF collection in communication with the surgical site. The pseudomeningocele had a large extracranial component and a relatively smaller intracranial component underlying the craniotomy site, causing mass effect on the underlying brain (figure 1B).
We performed a high-volume lumbar puncture and applied a pressure bandage over the site of the pseudomeningocele. He had an opening pressure of 14 cmH2O, 45 mL of CSF was drained and closing pressure was 8 cmH20. Following the lumbar puncture, over the next 48 hours, he developed focal seizures affecting his left arm and leg and progressive left upper and lower limb weakness. On examination, he had power 0/5 in his left lower limb and 3/5 in his left upper limb.
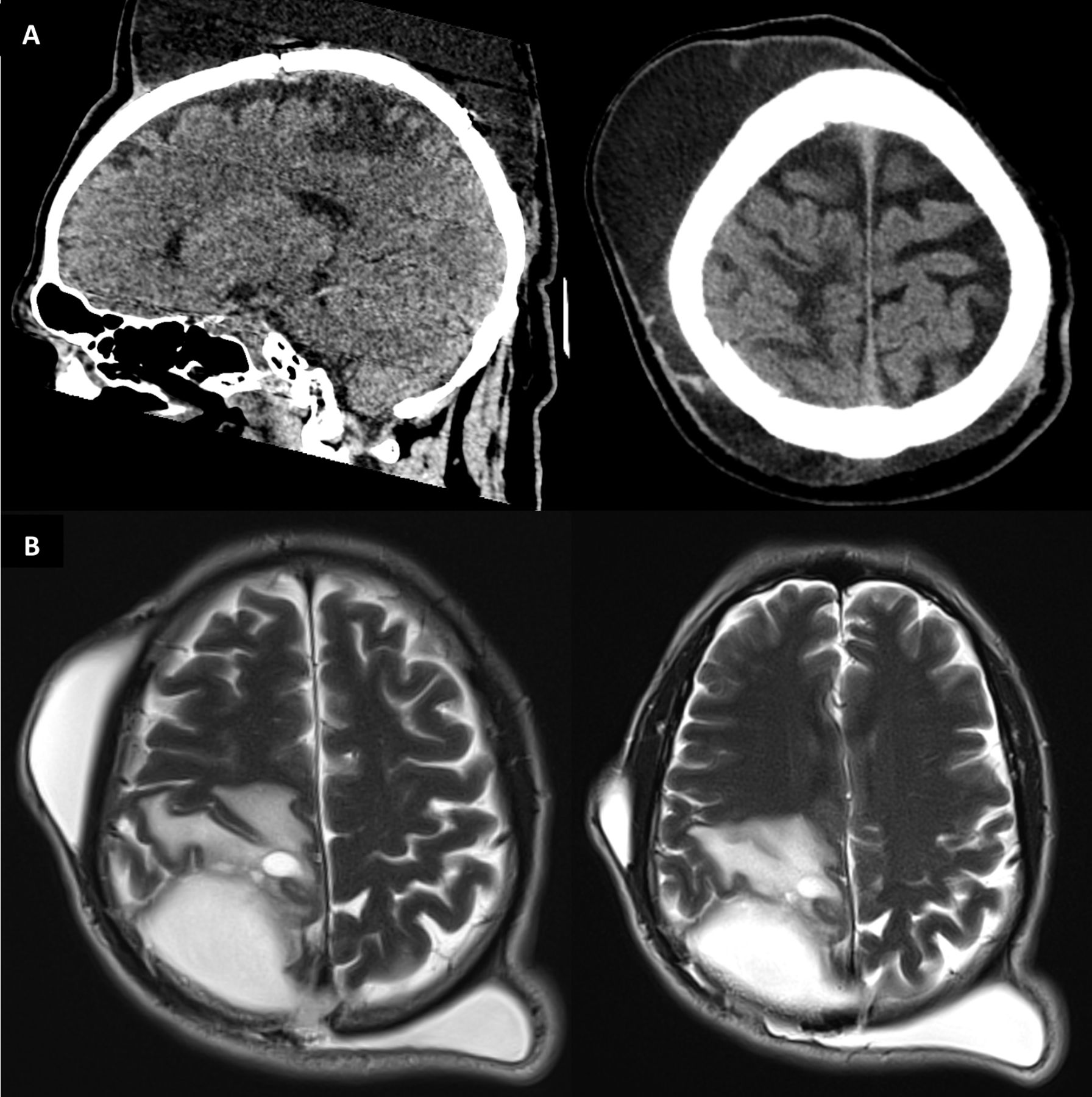
CT imaging demonstrated near complete resolution of the intracranial component of the pseudomeningocele; however, there was a new focal hypodensity in the underlying brain, suggestive of oedema (figure 2A). He was given high-dose steroids. MR imaging, obtained the following day, confirmed T2 high signal in the right post central gyrus, extending into the paracentral lobule and corona radiata representing oedema (figure 2B). There were no areas of restricted diffusion to suggest an infarction. The MRI also showed a recurrence of the intracranial component of the pseudomeningocele.

{kind=link}
{kind=link}
(A) CT following lumbar puncture, sagittal and coronal images demonstrating resolution of the intracranial component of the pseudomeningocele, expansion of the underlying brain with new areas of focal hypodensity. (B) Axial T2-weighted MRI images demonstrating high signal in the right post central gyrus, extending into the paracentral lobule and corona radiata representing oedema.
He had a right subgaleal-peritoneal shunt inserted for treatment of the giant pseudomeningocele. Over the next week, his left sided weakness and pseudomeningocele resolved and at discharge from hospital he was neurologically intact.
We postulate the high-volume lumbar puncture caused decompression of the intracranial component of the pseudomeningocele and rapid expansion of the underlying brain. This sudden reduction in pressure, likely resulted in a significant increase in local blood flow, subsequent venous congestion and vasogenic brain oedema. A similar pathophysiology has been suggested for postoperative intracranial hypotension-associated venous congestion (PIHV).2–4 We believe this case represents a spectrum of the same disease process. PIHV is extremely rare, but should be considered if patients develop unexpected neurological deterioration following loss of significant amounts of CSF.
Learning points
Most postoperative cranial pseudomeningoceles resolve spontaneously. Persistent giant cranial pseudomeningoceles are extremely rare.
Initial management options include observation, pressure bandage and lumbar cerebrospinal fluid (CSF) drainage.
If a patient develops unexpected neurological deterioration following loss of significant amounts of CSF, clinicians should consider postoperative intracranial hypotension-associated venous congestion as a possible cause.
Ethics statements
Patient consent for publication
Footnotes
Contributors KMR, CC and RB: patient management; drafted and final edit of the manuscript. JPL: analysed imaging data and provided images; edit of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.