Article Text

Statistics from Altmetric.com
Description
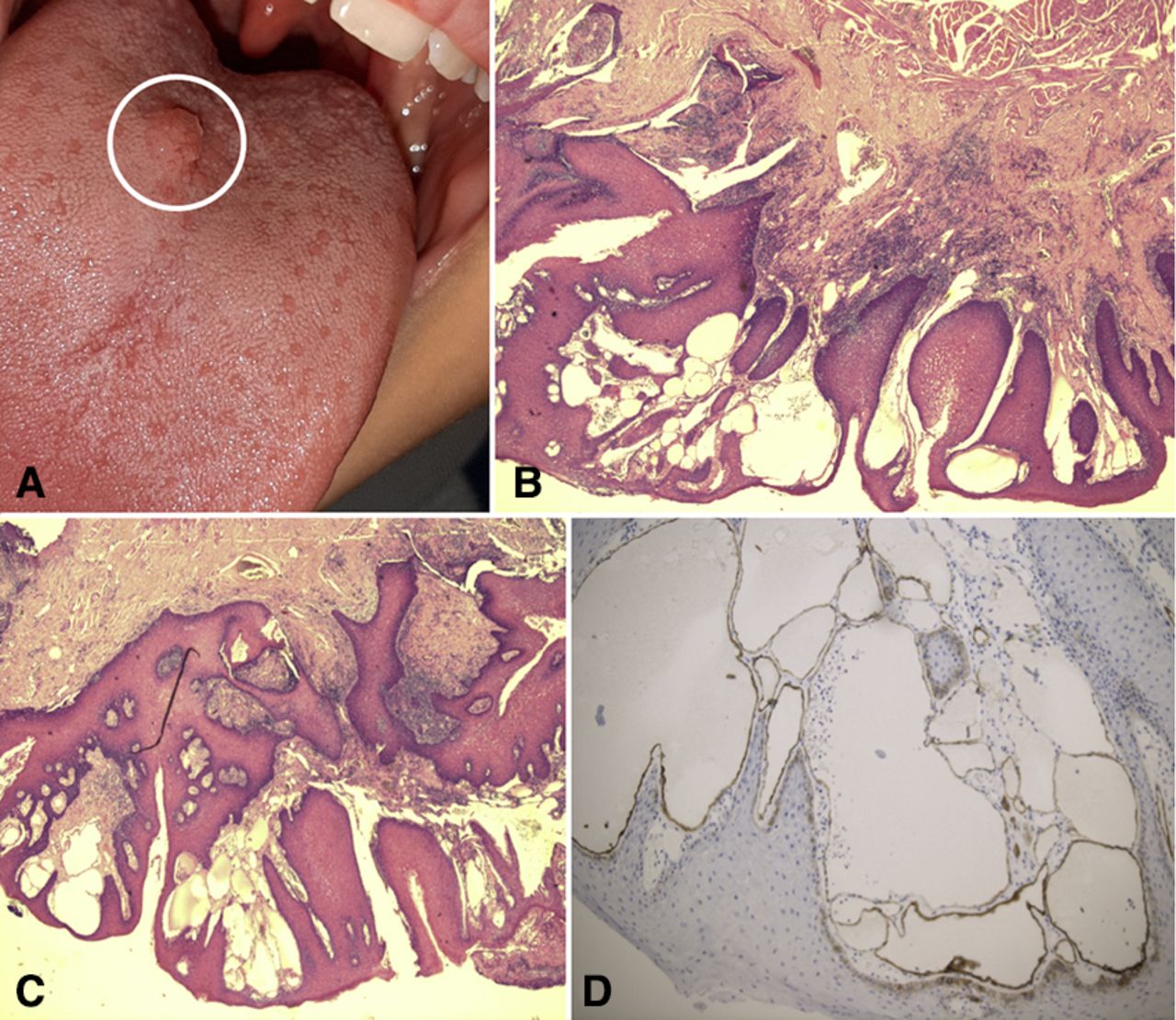
A 13-year-old boy, affected by cystic fibrosis, presented with a red, small lesion of the posterior part of the tongue (figure 1A). The lesion was 7×4 mm in size. The mass was slightly tender on palpation, firm and not bleeding on manipulation. The remaining physical examination was unremarkable. Under general anaesthesia, the patient underwent the removal of the lesion. The histopathological examination showed, at the H&E staining, a parakeratinised stratified squamous epithelium with enlarged blood vessels (figure 1B). Connective tissue revealed numerous large dilated blood-filled spaces lined by endothelial cells encircled by a chronic inflammatory infiltrate (figure 1C). Lymphatic vessels dilatation was also present (figure 1D). The final diagnosis of solitary angiokeratoma of the tongue was obtained.

{kind=link}
(A) Clinical picture showing the isolated swelling of the tongue. (B) Histopathological picture of angiokeratoma, H&E staining, revealing a parakeratinised stratified squamous epithelium with enlarged blood vessels; (C) large dilated blood-filled spaces lined by endothelial cells encircled by a chronic inflammatory infiltrate; (D) lymphatic vessels dilatation using CD31 as a marker.
Mibelli first described the first case of angiokeratoma, involving fingers and toes in an adult patient, in 1889.1 The angiokeratoma is a rare benign vascular lesion that usually involves arms and legs.2 The pathogenesis of angiokeratomas is still unknown. It has been reported congenital origin due to an overlying arteriovenous fistula, or traumatic pathogenesis with the onset of lymphangioma localised after local injuries.3 Usually, the lesion appears as well-demarcated swelling due to a large dilated blood vessel located in the subcutaneous tissue. The male/female ratio is 2:1. In the great part of cases, angiokeratoma appears as dark-red or blue-black, macular/papular lesions, which do not blanch on pressure. Oral involvement is frequently seen in syndromes such as Klippel-Trenaunay-Weber syndrome, Cobb syndrome and other mixed vascular malformations.3 Only eight cases of isolated angiokeratoma of the tongue in adult patients have been reported in the literature.2 To date, only four cases of angiokeratoma circumscriptum of the oral cavity in children have been described in the literature.4–6
Usually, the lesions are present since birth, but in some cases, may occur during childhood as in other cases and even in adulthood, especially in the case of traumatic aetiology. The natural course is usually benign, the only clinical features may be bleeding, discomfort or cosmetic alterations. Angiokeratoma appears in the oral cavity, often associated with systemic diseases and represents multiple papules in buccal mucosa and tongue causing dysphagia or drooling; but in our case, the patient has cystic fibrosis, which, upon reviewing the literature, seems not to have any relationship with the angiokeratoma.5 In our case, the lesion was solitary and there were no other lesions on the skin or in the oral cavity. The main differential diagnoses are haemangioma, lymphangioma and malignant melanoma.
Angiokeratoma may be treated with complete surgical excision, cryotherapy or laser ablation and no surgical complications have been reported in the literature or in our patient.6 7 Usually, no recurrences have been described but, recent reports suggest the possibility of a recurrence.7 In our case, after surgical excision, no recurrence is found after a 2-year follow-up. Isolated angiokeratoma of the tongue is a rare disease in children and, in most cases, this lesion may have a syndromic aetiology. Surgery is the treatment of choice to resolve both symptoms and histopathological diagnosis.
Patient's perspective
I am very happy about the care received by my son. I hope that the publication of this article will help other doctors and patients to recognize and treat this condition.
Learning points
Solitary angiokeratoma of the oral cavity is very rare in paediatric patients.
Localisation of the tongue is very infrequent.
Even in the presence of a solitary angiokeratoma of the tongue, the exploration of thorax, abdomen, arms and legs is mandatory to rule out the presence of syndromic diseases.
Ethics statements
Patient consent for publication
Footnotes
Contributors OA treated the patient and drafted the manuscript. FDC performed the pathological evaluation. FDP drafted and supervised the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.