Article Text

Abstract
The development of vaccinations has been instrumental in the ongoing effort to combat the COVID-19 pandemic. Although the benefits of vaccination are unquestionable, there have been reports of potentially rare life-threatening complications following vaccination including thrombocytopaenia, haemolytic anaemia, vasculitis and myocarditis. Haemophagocytic lymphohistiocytosis (HLH), a rare but life-threatening inflammatory condition, has also been described postadenoviral vector COVID-19 vaccination but it has never been reported post-messenger RNA (mRNA) COVID-19 vaccination. We report two cases of HLH admitted to our hospital after administration of COVID-19 mRNA vaccines. We also searched the vaccine adverse event reporting system and found 50 reports of suspected HLH following COVID-19 vaccination. Presently, we cannot define a causality between COVID-19 mRNA vaccination and HLH development. However, we hope the reporting of our two cases (and additional cases seen in the adverse event reporting database) will help us determine whether there is a potential relationship. Prompt recognition of this condition is of utmost importance to initiate life-saving therapy.
- COVID-19
- haematology (drugs and medicines)
- immunological products and vaccines
- haematology (incl blood transfusion)
- rheumatology
Statistics from Altmetric.com
- COVID-19
- haematology (drugs and medicines)
- immunological products and vaccines
- haematology (incl blood transfusion)
- rheumatology
Background
Over 200 million cases of COVID-19 infections have been confirmed worldwide. Multiple platforms were used to develop vaccine candidates, including messenger RNA (mRNA) vaccines encoding the SARS-CoV-2 spike glycoprotein. The mRNA vaccines, tozinameran and elasomeran, were approved by the US Food and Drug Administration (FDA) under emergency use authorisations; currently only tozinameran has full FDA approval. Both are highly efficacious in preventing serious outcomes, including hospitalisation, severe illness and death. Current knowledge about the safety of COVID-19 vaccines relies on data from phase 1–3 randomised controlled trials and vaccine safety surveillance systems.1 2 Due to the highly contagious nature of the disease and the pandemic straining healthcare systems, the benefits of mass vaccination efforts are unquestionable.3 Nonetheless it is important to recognise that similar to post-COVID-19 infectious complications, rare life-threatening complications post vaccination have also been reported including thrombocytopaenia, haemolytic anaemia, vasculitis and myocarditis.4–9
Haemophagocytic lymphohistiocytosis (HLH) is a rare, severe, uncontrolled hyperinflammatory reaction where activated lymphocytes and histiocytes infiltrate all organs and secrete large amounts of cytokines, leading to tissue damage and organ failure. Characteristic features include prolonged fever, splenomegaly, pancytopenia and haemophagocytosis. Biochemical markers include hyperferritinaemia, hypertriglyceridaemia and hypofibrinogenaemia. Due to its rarity and variable clinical presentation, an accurate diagnosis may be delayed, leading to substantial morbidity and mortality. Although HLH has been described post-Covid-19 infection as well as postadenoviral vector vaccination,10–14 it has never been reported post-mRNA vaccination. We report two cases of HLH admitted to our hospital from June to August 2021 after administration of mRNA vaccines. We also searched the vaccine adverse event reporting system (VAERS) (last release 09/10/21) for ‘HLH’ and found 50 reports of suspected HLH postvaccination.15 We cannot currently define a causal relationship between vaccination and the development of HLH, additional surveillance is needed to understand whether a relationship exists, if any, between them.
Case presentation
Patient 1 is a 60-year-old man with a history of Barrett’s esophagus who developed altered mental status and slurred speech 6 days after the first dose of tozinameran (BNT162b2 Pfizer-BioNTech vaccine). He was initially diagnosed with transient ischaemic attack, but progressively deteriorated over the next month developing fevers, drenching night sweats, loss of appetite, unintentional weight loss, delirium and became non-ambulatory.
Patient 2 is a 32-year-old woman with no prior medical history who developed high fevers 4 weeks after the second dose of tozinameran. She was briefly hospitalised at an outside hospital with new anaemia (haemoglobin 80 g/L), hyperferritinaemia (35 000 ng/mL) and elevated transaminases. Rheumatological, oncological and infectious workups were negative, and fevers worsened despite 8 weeks of prednisone 50 mg daily. By the ninth week of worsening symptoms as an outpatient, fevers reached 40°C and became debilitating. She was re-admitted and was transferred to our institution for further management. By this time her ferritin had increased to 68 212 ng/mL (normal range 15–150 ng/mL) and neopterin was 9.5 ng/mL (normal range <2.5 ng/mL).
Investigations
Acute COVID-19 infection was ruled out in both patients based on negative PCR tests of nasopharyngeal specimens. Negative nucleocapsid and positive anti-spike antibodies confirmed no prior COVID-19 infection.
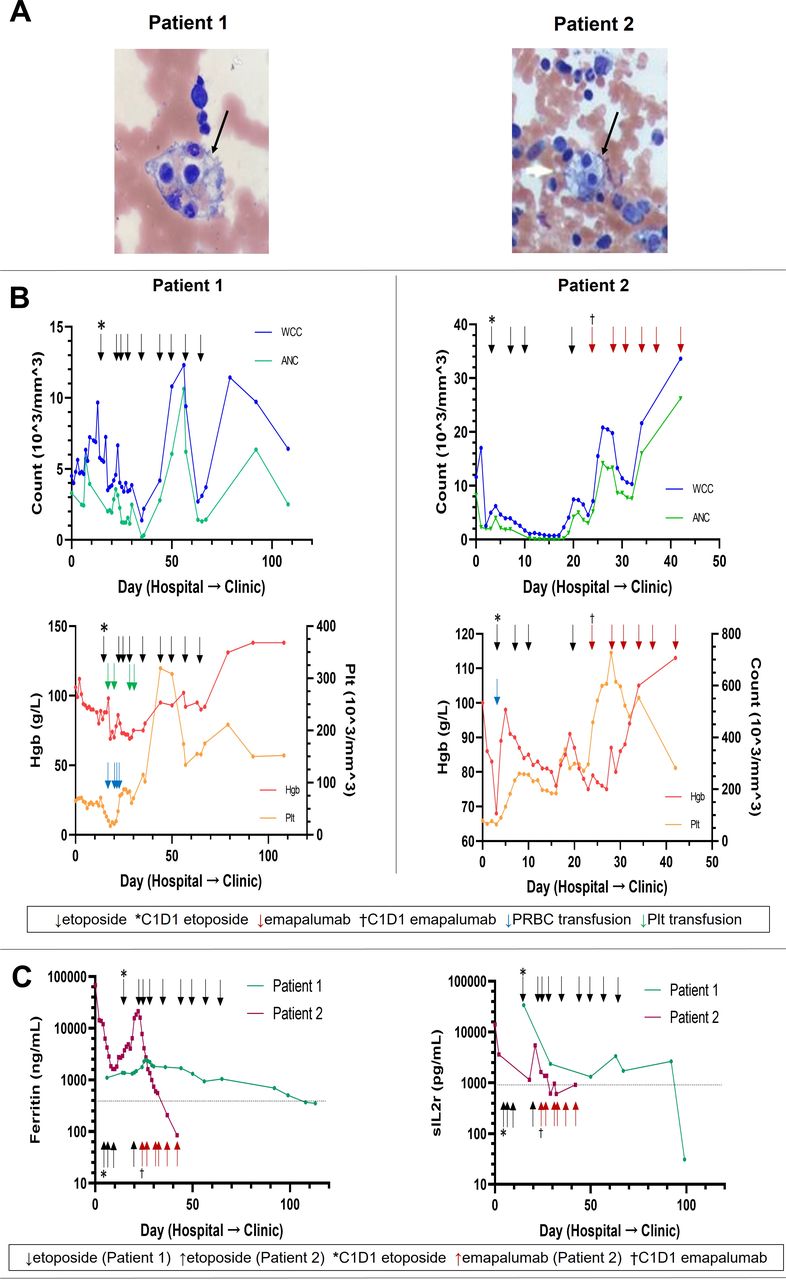
Patient 1 met 6/9 HLH criteria including a bone marrow biopsy that showed haemophagocytosis (table 1, figure 1A). Patient 2 met 7/9 HLH criteria including haemophagocytosis on bone marrow biopsy (table 1, figure 1A). The diagnosis of HLH was made in both patients based on these criteria. Table 1 details the extensive infectious, malignant and rheumatological workups that were obtained in both patients to rule out alternate aetiologies for HLH.
Patientcharacteristics and clinical data

{kind=link}
HLH post-COVID-19 vaccine. (A) Depicts bone marrow aspirate smears obtained by means of bone marrow biopsy in patient 1 and patient 2, which show haemophagocytosis (black arrow) in both patients. (B) Depicts trends in white cell count (WCC), absolute neutrophil count (ANC), haemoglobin (Hgb) and platelet (Plt) for patient 1 and patient 2. (C) Depicts trends in ferritin and soluble IL-2 receptor (sIL2R) on a logarithmic scale with dotted line indicating upper limit of normal for ferritin (400 ng/mL) and sILR (858 pg/mL). HLH, haemophagocytic lymphohistiocytosis.
Differential diagnosis
The differential diagnosis was very broad in both patients. Table 1 lists the complete work up for each patient, which aimed to rule out not only an aetiology for their fevers but also an underlying aetiology that could result in secondary HLH. Given their high fevers, infectious aetiologies were high on the differential for both patients. In addition to blood cultures and ruling out SARS CoV-2 infection, evaluation for Aspergillus, Babesia, Bartonella, Brucella, Leptospira, Tuberculosis and Francisella tularensis in the serum were performed. Both patients also had lumbar punctures to evaluate for bacterial, fungal and viral aetiologies; studies included evaluation for Cryptococcus, Epstein-Barr virus, cytomegalovirus and West Nile virus.
When infectious aetiologies were negative, both patients also underwent an extensive rheumatologic workup which included evaluation for systemic lupus erythematosus, mixed connective tissue disorder and vasculitis.
CT, including positron emission tomography CT, was also performed to evaluate for oncological explanations for their symptoms. Although lymphadenopathy was seen in both patients, biopsies of suspicious lymph nodes were non-diagnostic for malignancy. Additionally, both patients had bone marrow biopsies as part of the workup for fever of unknown origin, both to evaluate for HLH as well as to rule out a haematological malignancy which subsequently revealed evidence of haemophagocytosis. A final diagnosis of HLH was even more suggestive following drastic clinical response to HLH-directed treatment as well as further serological testing (elevated CXCL9, neopterin).
Treatment
Patient 1 was initially treated with 5 days of prednisone 1 mg/kg prior to the diagnosis of HLH but his symptoms were refractory to this treatment, and he continued to deteriorate. He was subsequently started on HLH-directed therapy with etoposide and dexamethasone.
Patient 2 had initial improvement in her symptoms and pancytopenia after starting etoposide and dexamethasone but after her fourth etoposide dose she developed neutropenic fevers and haemodynamic instability without identifiable infectious source. Due to concern for disease refractoriness, she was started on emapalumab-lzsg.
Outcome and follow-up
Patient 1 had dramatic improvement in his speech, ambulation and pancytopenia within 48 hours of starting etoposide and dexamethasone (figure 1B,C). He was discharged 13 days after his first etoposide dose and he initially continued to improve on outpatient follow-up visits, however, symptoms (night sweats, malaise) relapse and his HLH biomarkers worsen (worsening thrombocytopaenia, rising triglycerides, elevated ferritin) anytime he is tapered off steroids. He has been started on cyclosporine without meaningful improvement, so we have restarted steroids.
Patient 2 similarly had rapid improvement in her symptoms and laboratory markers after starting second line HLH-directed therapy. She was discharged home after 5 weeks and continues to improve on outpatient follow-up visits. She completed eight treatments of emapalumab-lzsg and on discontinuation, laboratory markers worsened, so we plan for a longer course of emapalumab-lzsg.
For patient 1, we considered intrathecal methotrexate as treatment for the neurological manifestations of HLH. Although intrathecal therapy has been used in thrombocytopenic patients, there is no consensus on a safe cut-off value of platelet counts. The patient had profound thrombocytopaenia (<20 000/µL), which was unresponsive to platelet transfusions during his hospital course. Given the risks of haemorrhagic complications, we were unable to offer this therapeutic intervention during the hospitalisation. Additionally, his neurological symptoms improved rapidly with systemic first line treatment for HLH with etoposide and steroids.
For patient 2, we discussed pursuing an allogeneic haematopoietic stem cell transplant as she initially had worsening laboratory HLH markers after emapalumab was being tapered. We are currently awaiting results of genetic testing to rule out hereditary HLH mutations that may have predisposed her to developing HLH before we subject her to transplant considering that she is being weaned off the emapalumab. Her biomarkers have also improved with prolonged emapalumab so we have currently deferred pursuit of transplant.
Elevated D-dimer can also be seen in HLH as many patients will have hepatitis and abnormal coagulation parameters. Although D-dimer is not included in the diagnostic criteria for HLH, it may be of interest to trend this lab to evaluate for response to HLH directed therapy.
Discussion
Over 350 million mRNA-vaccine doses have been administered in the USA without reported cases of HLH post-mRNA vaccination in the literature.16 In addition to our two patients, we found 48 additional reports of HLH following COVID-19 infection in the VAERS database (table 2 and online supplemental table S1). There were 25 females/25 males with a median age of 58-years-old. The distribution of vaccines was Pfizer (34), Moderna (14) and Janssen (2). Symptoms developed a median of 8 days (0–61 days) post first (22) and second (24) dose. All but one case required hospitalisation (median 14 days). At the time of the reporting, only 20% had recovered and seven patients had died. It is unclear if all patients met criteria for HLH with several reports indicating an alternative diagnosis was suspected.
Supplemental material
Reported cases of HLH related to SARS/CoV-2 vaccine to the VAERS database
Vaccination remains one of our most effective public health tools in the setting of an ongoing worldwide pandemic. The potential relationship between COVID-19 vaccination and development of HLH warrants further investigation. Although review of the literature reveals HLH following COVID-19 infection10–12 and post-COVID-19 adenoviral vector vaccination,13 14 this is the first report of patients developing HLH post COVID-19 mRNA vaccination. In two cases of HLH following ChAdOx1-S (recombinant) (AZD1222), patients were refractory to first line HLH directed therapy and responded to administration of anakinra, an interleukin-1 receptor antagonist.14 In our report, patient 2 had a short response to etoposide and steroids but became refractory and required administration of emapalumab-lzsg with clinical improvement.
Our report is limited by its retrospective approach, the self-reported nature of VAERS data, and lack of access to primary vaccine trial data and to the VAERS reporters to confirm the HLH diagnoses. VAERS cases may initiate investigations into potential associations between a vaccine and adverse events, but on their own cannot prove causality. Pharmacovigilance is therefore key to determine the true incidence of these exceedingly rare toxicities considering that millions of doses of the various available vaccines have been safely administered worldwide. We hope that our two cases of HLH raise awareness of a potential unexpected adverse effect associated with COVID-19 mRNA vaccines as prompt recognition of this condition is of utmost importance to initiate life-saving therapy.
Patient’s perspective
Patient 1
This has been the most incredibly painful and difficult 6 months of my family life. All of my health issues began after my vaccination and my health declined at a rapid rate. There was no progress or understanding of what was causing this deterioration and I felt my life was in severe danger.
After being diagnosed with HLH my life turned around. Starting the medications for HLH has helped me. I am looking towards many years of good health. I feel very strongly that the medical community should know my story in case it could save someone else’s life.
Patient 2
I almost died because of HLH especially since the traditional chemotherapy did not work for me. I feel very lucky to have received the targeted medicine so that I could get my life back and live again. I am still on my way to recovery but I am definitely getting better everyday and keeping my fingers crossed for a full recovery.
Learning points
Clinicians should maintain a high level of suspicion for haemophagocytic lymphohistiocytosis (HLH) in patients who present with non-specific symptoms of cytokine storm and multiorgan failure without an identifiable infectious, malignant or rheumatological aetiology. Due to the rarity and variable clinical presentation of HLH, an accurate diagnosis may be delayed, leading to substantial morbidity and mortality.
This is the first report of HLH developing in two patients post-COVID-19 messenger RNA (mRNA) vaccination in the absence of other identifiable causes of HLH. Further investigation is needed to understand the relationship between COVID-19 mRNA vaccines and development of HLH.
HLH and other adverse events reported after COVID-19 mRNA vaccination remain extremely rare and should not diminish the well-documented safety profile of mRNA vaccines.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors VW and JCB designed the research. VW, CL, AH and JCB contributed equally to performing the research, analysing the data and writing the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests VW, CL and AH declare no conflicts of interest. JCB has served on advisory boards for Janssen, Pharmacyclics/AbbVie, BeiGene, AstraZeneca, Innate Pharma and receives institutional research support from Oncternal, Velosbio, Pharmacyclics/Abbvie and Acerta/AstraZeneca. She has received honoraria from Janssen.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.