Article Text

Statistics from Altmetric.com
Description
A 40-year-old man with an unremarkable medical history presented with a 1-year history of jaw and proximal muscle fatigue. He reported gaining 5 kg over the previous 2 months but had no fever, temporal headache, muscle pain, diplopia, eyelid ptosis, dysphagia, skin symptoms, cold intolerance, constipation or depression. His vital signs were normal. His speech was slow, and he spoke with a deep, muted, nasalised voice (video 1). His GRBAS (Grade, Rough, Breathy, Asthenic, Strained) Scores were G0, R1, B3, A3 and S0.1 He complained of masseter muscle fatigue after 18 s of gum chewing. His proximal muscle power was within normal limits.
ECG showed sinus rhythm and no ST changes. Laboratory evaluation revealed elevated creatine kinase and total cholesterol levels. Thyroid function tests showed free T4 and thyroid-stimulating hormone levels of 0.14 ng/dL (normal range: 0.90–1.70 ng/dL) and >100 µIU/mL (normal range: 0.35–4.94 µIU/mL), respectively. Tests for anti-thyroid peroxidase and anti-thyroglobulin antibodies were both positive. Based on these findings, he was diagnosed with Hashimoto thyroiditis and was started on levothyroxine sodium 50 µg daily. One week after, the dose was increased to 75 µg daily and continued for few months. Six weeks later, his thyroid hormone levels normalised, his symptoms improved and his speech rate and voice quality improved (video 1). However, his weight did not decrease. Due to the misalignment of these phenomena, it was unclear whether the weight gain was related to his hypothyroidism.
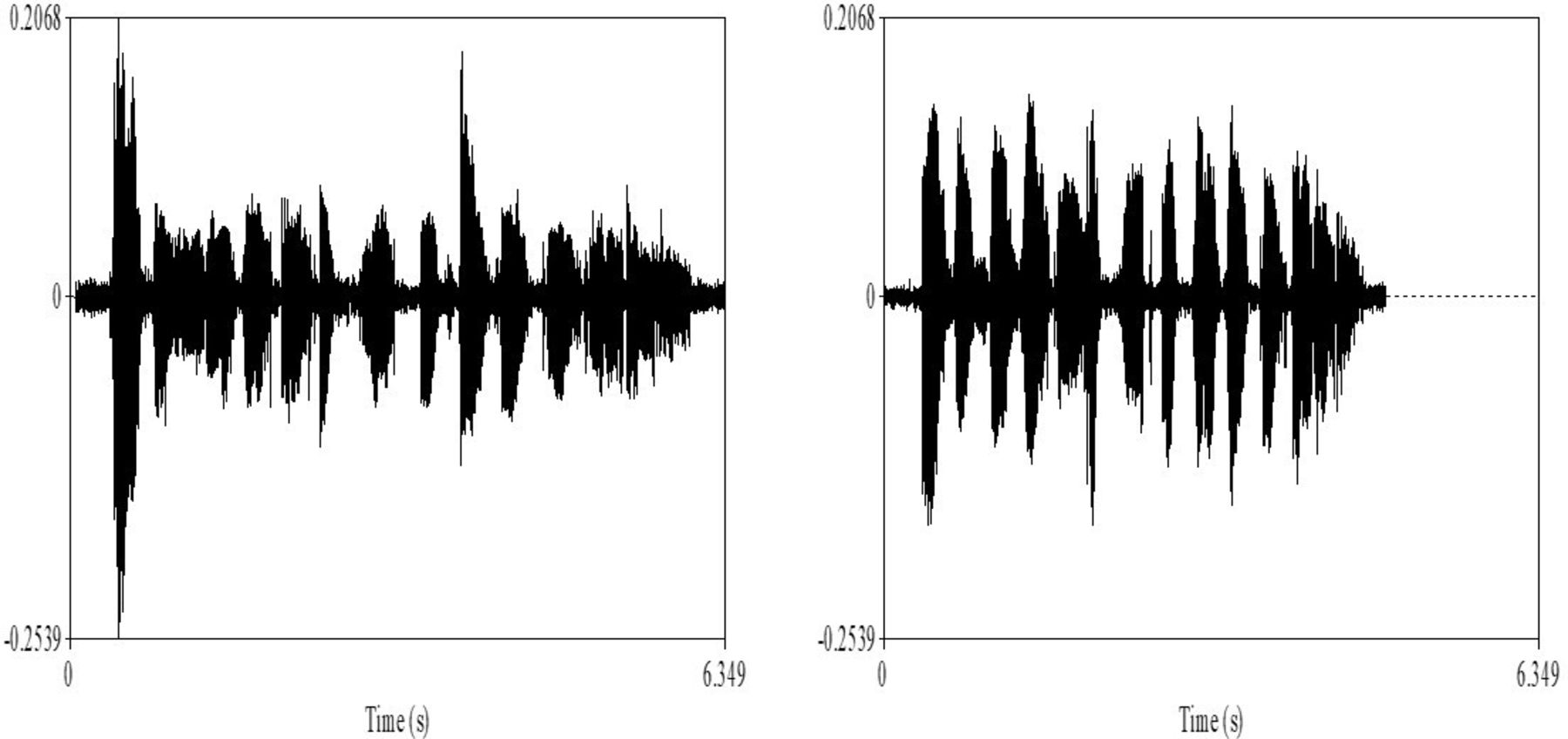
Using Praat speech analysis software, we analysed the patient’s speech before and after treatment (figure 1).2 The voice sample was taken in a closed examination room to avoid ambient sound.

{kind=link}
Using Praat, a free software program for speech analysis, we analysed the patient’s speech before and after treatment. Speech analysis comparing before (left) and after (right) the treatment of hypothyroidism. The vertical axis of the figure shows amplitude, and the horizontal axis shows time.
His pretreatment speech was slow (6.349 s), low-pitched (mean 90.28 Hz) and had a low-intensity (mean 58.33 dB); however, after 6 weeks of treatment, his speech became faster (4.859 s), had a higher frequencies (mean 96.21 Hz) and his speech intensity improved (mean 62.34 dB).
The differential diagnosis of nasal voice includes allergic diseases, upper respiratory tract infections and tumours of the nasal cavity and the sinuses. A history of allergies and recent infections should be obtained, and if a tumour lesion is suspected, anterior rhinoscopy should be performed. However, these diseases do not cause jaw and proximal muscle fatigue or weight gain. In cases of nasal slowed voice with elevated creatine kinase, myocarditis or viral myositis should also be considered. In addition, when elevated creatine kinase and cholesterol are present, acute myocardial infarction should be ruled out.
We hope that this description of the speech characteristics associated with hypothyroidism will help practitioners identify patients with undiagnosed or poorly managed hypothyroidism in clinical practice. Clinicians should suspect hypothyroidism in patients with slow speech and deep, muted and nasalised voices.3 4
Learning points
The differential diagnosis of nasal voice includes allergic diseases, upper respiratory tract infections, tumours of the nasal cavity and the sinuses and hypothyroidism.
Clinicians should suspect hypothyroidism in patients with slowed speech and a thick, low and nasal voice.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Footnotes
Contributors KK and SU identified significance. SU and KK wrote the manuscript. TT and TS revised it. All authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.