Article Text

Statistics from Altmetric.com
Description
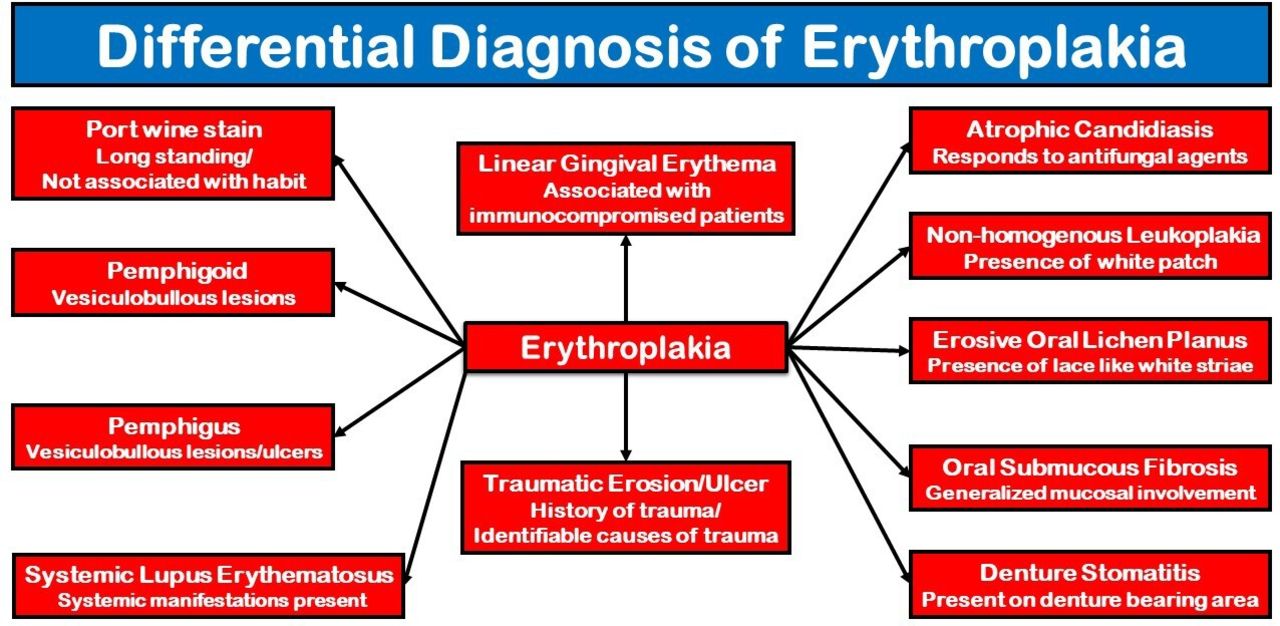
Erythroplakia is a rare oral lesion that presents as a well-defined, velvety-textured, homogenously red patch considered a potentially malignant disorder.1 Oral erythroplakia needs to be differentiated from other erythematous oral lesions, especially of inflammatory origin, often by histopathological evaluation. It has been emphasised that a persistent asymptomatic oral erythroplasic patch when present in high-risk sites such as the ventral surface of the tongue or the floor of the mouth may be the earliest and primary sign of oral cancer.2 The middle-aged and the elderly are usually affected, with a slight male gender predilection. The prevalence is only about 0.02%–0.2%. The aetiopathogenesis is unclear, yet a strong association with usage of tobacco and alcohol has been cited in the literature.1 In about 85% of cases, histological signs of squamous cell carcinoma are seen on histological evaluation.2 Erythroplakia is generally a diagnosis of exclusion and needs to be differentiated from other red oral lesions (figure 1), such as erosive oral lichen planus, erythematous candidiasis, oral mucositis, pemphigus vulgaris, mucous membrane pemphigoid and systemic lupus erythematosus, with biopsy performed in addition to a thorough history-taking session and meticulous clinical examination.3

Flow diagram showing the differential diagnosis of oral erythroplakia.
A 51-year-old male patient reported with burning sensation in the tongue for 2 months. His medical history was unremarkable, with a history of chronic use of smoking tobacco and drinking alcohol. A well-demarcated, irregular, erythematous patch was seen on the left side of the dorsum of the tongue crossing the midline, almost homogenously red in colour, measuring about 5×3 cm in size, with smooth surface and velvety texture, raised everted borders laterally, rough, indurated in consistency, and slightly tender on palpation (figure 2). A provisional diagnosis of erythroplakia with oral squamous cell carcinoma was made and an incisional biopsy was performed. Histological evaluation revealed hyperplastic, stratified squamous epithelial cells and infiltration of malignant epithelial cells in the connective tissue stroma with keratin pearl formation, suggestive of well-differentiated squamous cell carcinoma (figure 3). The patient was then referred to a surgical oncologist, underwent surgery and radiotherapy, but was subsequently lost to follow-up.
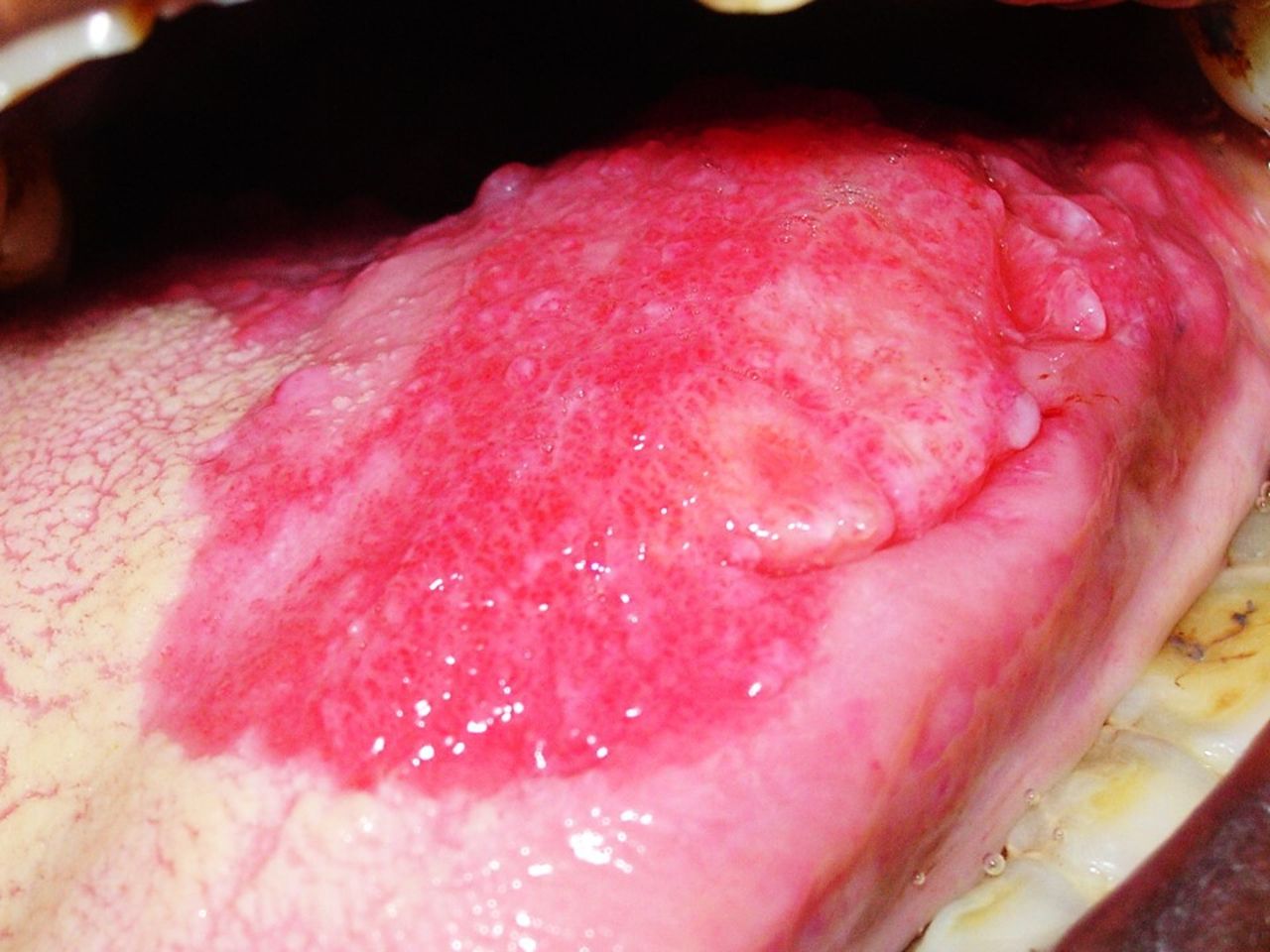
An irregular erythematous patch seen on the left side of the dorsum of the tongue with raised indurated borders medially.

{kind=link}
{kind=link}
{kind=link}
Squamous cell carcinoma.
Learning points
Oral erythroplakia is a rare lesion.
It is the oral potentially malignant disorder with the strongest malignant potential and is often histologically diagnosed as squamous cell carcinoma.
An idiopathic red lesion in the oral cavity needs to be histologically evaluated.
Ethics statements
Patient consent for publication
Footnotes
Contributors RD examined the patient. PB performed the biopsy. NM interpreted the histological findings. SRM prepared the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.