Article Text

Statistics from Altmetric.com
Description
A 28-year-old female patient who did not have any systemic disease before presented with complaints of sudden onset of abnormal jerky movements of all limbs along with tongue bite lasting for about 10 min. She had history of caesarean section 1 week back. Neurological examination revealed no focal neurological deficit. Her routine blood investigations and cerebrospinal fluid analysis were normal. MRI of brain showed areas of altered signal intensity (areas of T2 and FLAIR hyperintensities) involving bilateral basal ganglia, along cortical and subcortical regions predominantly along posterior aspect involving bilateral parieto-occipital lobes and left frontal lobe representing vasogenic oedema. There was also involvement of left cerebellar region and vermis (figure 1). These MRI changes were suggestive of vasogenic oedema secondary to cerebrovascular autoregulatory dysfunction which was consistent with the diagnosis of postpartum central variant of reversible encephalopathy syndrome (PRES).1 2 The patient was treated with intravenous levetiracetam, intravenous phenytoin and supportive care, she responded well to treatment and did not have any further seizures or neurological issues. Repeat MRI brain on follow-up after 8 weeks revealed near complete resolution of the lesions (figure 2).
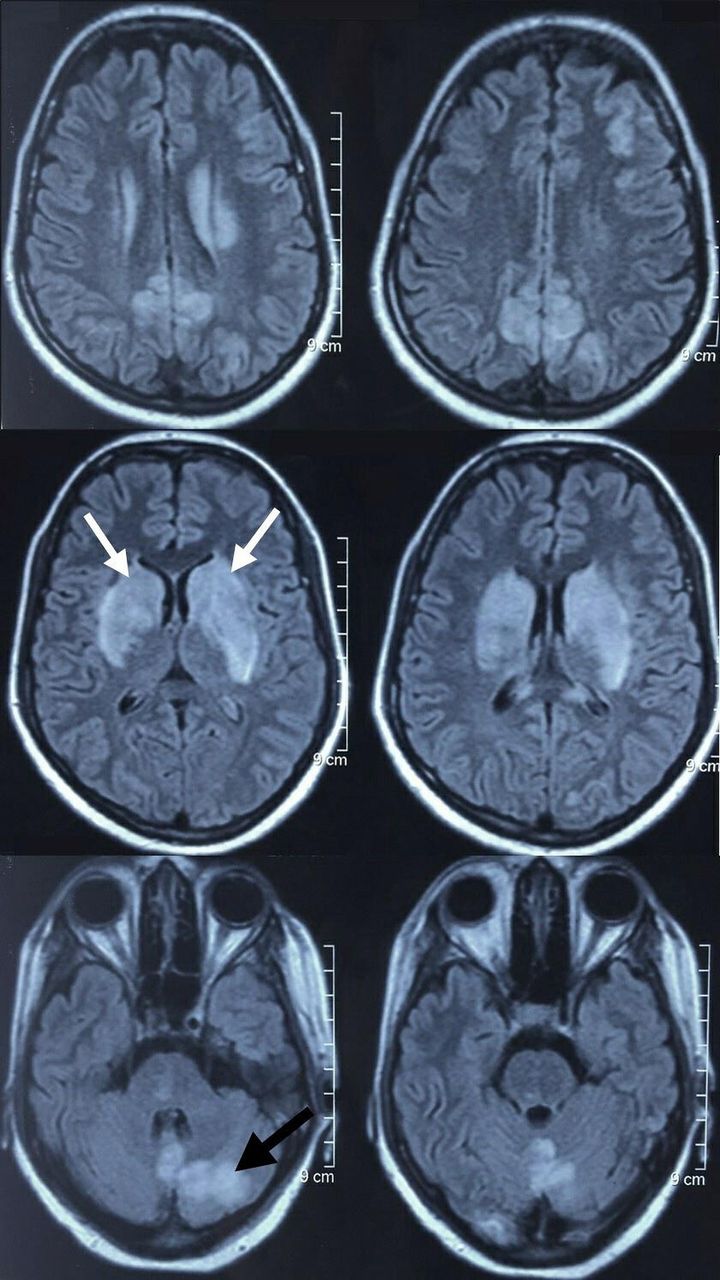
MRI of brain showing areas of altered signal intensity (areas of T2 and FLAIR hyperintensities) involving bilateral basal ganglia (white arrows), along cortical and subcortical regions predominantly along posterior aspect involving bilateral parieto-occipital lobes, left frontal lobe left cerebellar region (black arrow) and vermis.

{kind=link}
{kind=link}
Repeat MRI brain on follow-up after 8 weeks showing near complete resolution of the lesions.
The central variant of PRES has been described in past as ‘hypertensive brainstem oedema encephalopathy’, ‘hypertensive brainstem encephalopathy’, ‘reversible pontine oedema’, ‘reversible brainstem hypertensive encephalopathy’ or ‘brainstem hyperintensity in arterial hypertension’.3 These labels are confusing because PRES doesn’t need hypertension as a cause and it is not limited solely to brainstem involvement. Hence it is proposed that terms like ‘central variant PRES’ or ‘central reversible encephalopathy syndrome’ are more appropriate, particularly because central structures other than the brainstem can also be involved in this variant. Central variant PRES was reported for the first time in 2010 the setting of systemic lupus erythematosus.4 There are no established risk factors which predispose patients to atypical variant of PRES. As per available literature, the differential diagnosis for current case included inflammatory demyelination, osmotic myelinolysis syndrome, infiltrative glioma, lupus-associated central nervous system vasculitis, reversible cerebral vasoconstriction syndrome and rhomboencephalitis.5 The pathophysiological process in central variant PRES is suggested to be the endothelial cell dysfunction occurring within smaller, perforating vessels supplying the brainstem and basal ganglia.3
Learning points
Posterior cerebral distribution of reversible encephalopathy syndrome (PRES) has been well known but one needs to be aware of its central variant
This entity is largely reversible, hence utmost care should be taken to avoid misdiagnosis and inappropriate management of central variant of PRES.
Ethics statements
Patient consent for publication
Footnotes
Contributors DMC prepared the manuscripts and collected the MRI. PNR provided the clinical data of the patient and served as primary neurologist. NG provided the detailed radiology inputs. AM supervised the study concept and reviewed the manuscript and image findings of the case.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.