Article Text

Statistics from Altmetric.com
Description
A man in his mid-20s called Emergency Medical Services (EMS) to report that he ingested 25 g of sodium nitrite in a suicide attempt. The paramedics found the patient somnolent with systolic blood pressure 110 mm Hg, heart rate 130 bpm, oxygen saturation 79% with notable cyanosis and diaphoresis. EMS reported a scale and white powder at the scene. He was intubated after a tonic-clonic seizure, developed ventricular fibrillation, defibrillated at 200 J, and Cardiopulmonary Resuscitation (CPR) was initiated as the cardiac rhythm degraded to pulseless electrical activity. Intravenous medications administered included 2.5 mg epinephrine 1:10 000, 1 g calcium chloride, 100 mEq sodium bicarbonate 8.4% and 5 g hydroxocobalamin.
The patient was transported to the emergency department (ED) with ongoing CPR. On hospital arrival in the ambulance bay, the paramedics were given 100 mg methylene blue to administer intravenously as they did not have the antidote in their ambulance. During the primary survey in the ED, he was in asystole, with end-tidal CO2 12 mm Hg and blue-grey discolouration of the skin. The patient received intravenous 2 mg epinephrine, 1 g calcium chloride, 50 mEq sodium bicarbonate 8.4%, 50 mg methylene blue and 125 mL intralipid. Arterial blood gas was obtained with notable brown-black appearance (figure 1) and pH 7.03, PCO2 87 mm Hg, PaO2 2 mm Hg, bicarbonate 22 mmol/L, lactate 30 mmol/L. The haemoglobin was 12.4 g/dL with 28.8% methaemoglobin (reference range 0.4%–1.5%). Resuscitation was ceased 50 min after the initial arrest. Postmortem-combined nitrate and nitrite level was 5300 µmol/L (reference range 0–53) and autopsy revealed brown discolouration of muscle tissue consistent with methaemoglobinemia (figure 2).

Arterial blood gas syringe containing brown-black blood seen in methaemoglobinemia.

Brown discolouration of muscle tissue from fatal sodium nitrite exposure on left, compared with normal muscle appearance on right.
Sodium nitrite is commonly used in food preservation and in treating cyanide toxicity. It is a powerful oxidative agent, which oxidises haemoglobin to methaemoglobin, reducing oxygen carrying capacity of erythrocytes and causing tissue hypoxia.1 2 Clinical manifestations of sodium nitrite toxicity include hypotension, hypoxemia, encephalopathy, dysrhythmia and cardiac arrest.1 3 Chocolate-coloured blood may be noted during intravenous access and phlebotomy. Arterial blood gas measurements may show a normal PaO2 due to electrochemical measurement of dissolved oxygen in blood, rather than the oxygen associated with haemoglobin, although co-oximetry will yield an elevated methaemoglobin concentration.1 Hydroxocobalamin administration, which was given by EMS for possible cyanide toxicity, may have interfered with co-oximetry testing given its strong colour and absorbance. Despite this, the diagnosis is clear when considering the initial patient report of sodium nitrite ingestion, his clinical presentation, profound acidaemia and nitrite test results.4
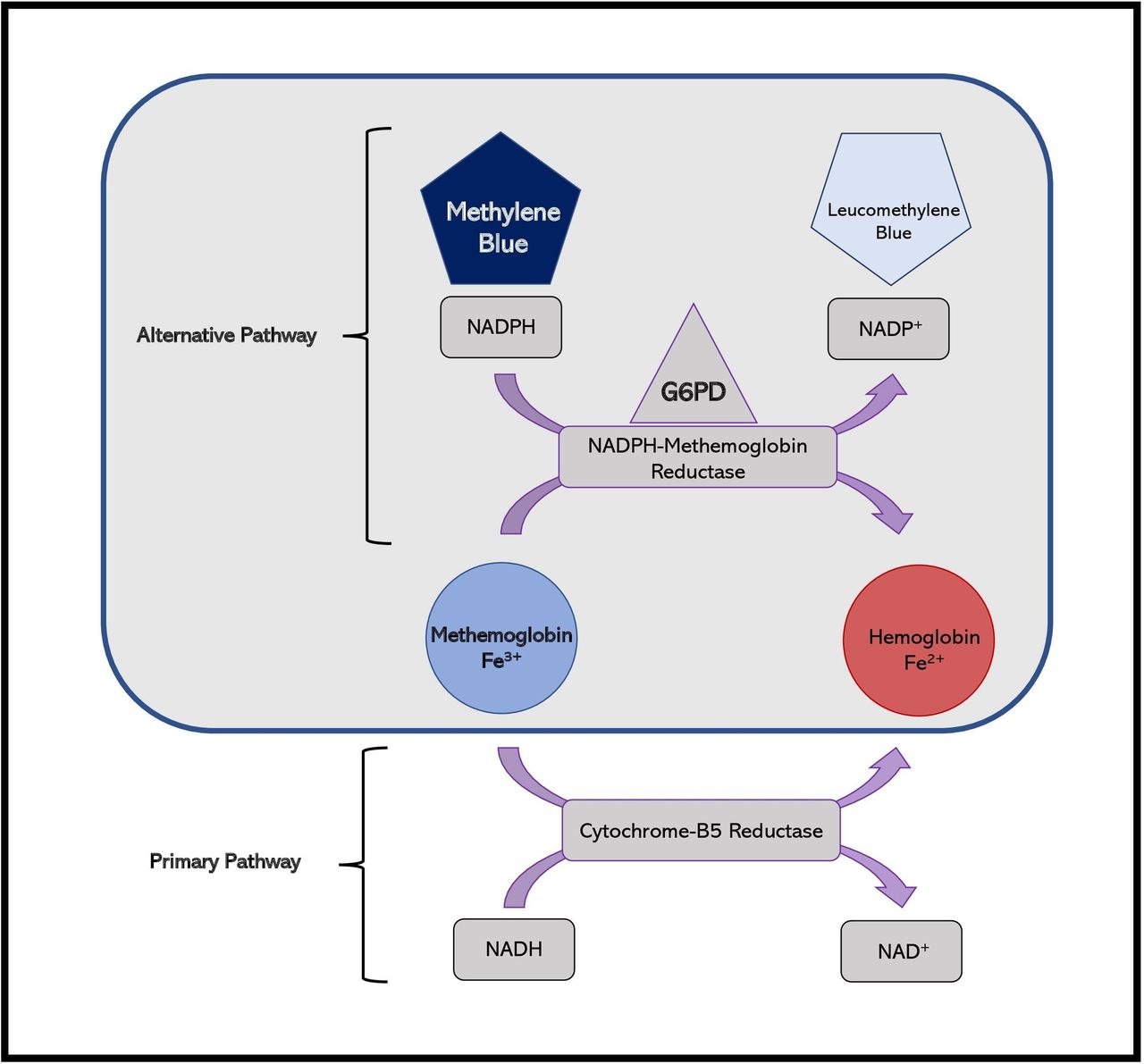
Methylene blue is the mainstay of treatment for methaemoglobinemia and is dosed 1–2 mg/kg, infused over 5 min and can be repeated if symptoms persist.1 Methylene blue is a catalyst for reducing methaemoglobin to haemoglobin within erythrocytes, via the enzyme NADPH-methaemoglobin reductase (figure 3).2 Additional treatment approaches include ascorbic acid, hyperbaric oxygen, exchange transfusion and extracorporeal membrane oxygenation.3 5
{kind=link}
{kind=link}
{kind=link}
Reduction of methaemoglobin to haemoglobin via the primary pathway, catalysed by cytochrome-B5 reductase (below), in contrast to the methylene blue-dependent alternative pathway via NADPH-methaemoglobin reductase (above). Activation of the alternative pathway requires methylene blue as a cofactor, in the presence of adequate glucose-6-phosphate dehydrogenase (G6PD). Figure created by authors.
Although unintentional sodium nitrite poisoning has been previously reported from home-cured meats and contaminated well-water, intentional ingestion of sodium nitrite for suicide has been increasingly reported.6–10 One case series of five patients with methaemoglobinemia in New York identified improperly labelled sodium nitrite salt as the culprit, with measured levels of sodium nitrite in the food exceeding 3000 parts per million; the US Food and Drug Administration legal limit for sodium nitrite in prepared meats is 200 parts per million.7 The reported lethal dose of ingested sodium nitrite has ranged from 0.7 g to 6 g.11 Sodium nitrite is readily available as pure granules via online retailers and its use in suicide has been discussed in online forums.8 9 Given this concerning trend in increasing rates of fatal sodium nitrite ingestions, it is essential for EMS providers and emergency clinicians to recognise methaemoglobinemia for prompt treatment.
Learning points
Sodium nitrite ingestion can be a fatal cause of methaemoglobinemia and should be considered based on cyanosis, hypoxemia and dark appearance of blood on venipuncture.
High clinical suspicion and early administration of methylene blue is essential to treatment of this life-threatening condition.
Sodium nitrite is an emerging cause of intentional ingestion for self-harm and important for front-line clinicians to recognise.
Ethics statements
Patient consent for publication
Footnotes
Contributors ZSW was the resident physician overseeing the patient’s care in our emergency department and was the primary author of the manuscript. NAY was the medical examiner and contributed to the writing and revision of the manuscript. SS was the attending physician for the patient’s care and contributed to the writing and revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.