Article Text

Abstract
Granular cell tumours (GCTs) are benign tumours that rarely develop in intraocular regions. We report a rare case of intraocular GCT in the ciliary body. A woman in her 20s with a history of bone marrow transplantation for malignant lymphoma in early childhood was referred to our department for bilateral proliferative diabetic retinopathy. A yellowish-white ciliary tumour was observed in the temporal periphery of the patient’s left eye during routine ophthalmological examination. As the tumour enlarged, we performed total resection combined with vitrectomy, silicone oil tamponade and cataract surgery. Histopathological examination revealed tumour cells with small, round or oval nuclei with eosinophilic cytoplasm. Positive immunohistochemical staining for S-100 and vimentin led to a diagnosis of ciliary GCT. No retinal detachment, proliferative membrane formation or tumour recurrence was observed 4 years postoperatively. Intraocular GCT should be considered a differential diagnosis of ciliary tumours.
- Retina
- Iris
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Granular cell tumours (GCTs) are rare, benign, solitary, painless and slow-growing tumours that develop in various tissues, but are mainly found in the skin and subcutaneous tissues of the head and neck in adults. GCTs usually develop during the fourth to sixth decades of life, with a female predilection.1 Approximately 3% of GCTs develop in the periocular region, that is, the orbit,1–5 extraocular muscles,6 7 lacrimal tissues,8 9 eyelid,10 conjunctiva11 and caruncle.12 However, intraocular GCTs are extremely rare, and only three cases in the anterior uvea and iris,13 retina14 and subretinal space15 have been reported. Here, we report a case of a ciliary GCT diagnosed based on the pathological examination of a total excision specimen.
Case presentation
The female patient in this case was in her 20s. During infancy, she developed T-cell lymphoma (stage IV). Two years later, bone marrow metastasis occurred, and she underwent bone marrow transplantation. Nine years later, she was diagnosed with a cerebral cavernous haemangioma. Three years thereafter, she developed primary ovarian insufficiency, slowly progressive type 1 diabetes, growth hormone deficiency, gout, hypertension, fatty liver disease and diabetic retinopathy. Few months prior to the index case, hyperthyroidism and thyroid nodules were detected, and the patient was diagnosed with an autonomously functioning thyroid nodule based on tissue biopsy findings. There was no significant family history of any of her disorders.
The patient was referred to our department due to vision loss in her right eye. Her corrected visual acuity was 20/600 in the right eye and 20/22 in the left eye. The right eye had vitreous haemorrhage due to proliferative diabetic retinopathy. In addition, she had severe diabetic retinopathy in her left eye. At the time of presentation, a yellowish-white elevated lesion that measured two times the diameter of the optic disc was observed in the temporal periphery of her left eye on indirect funduscopy, and a benign ciliary tumour was suspected.
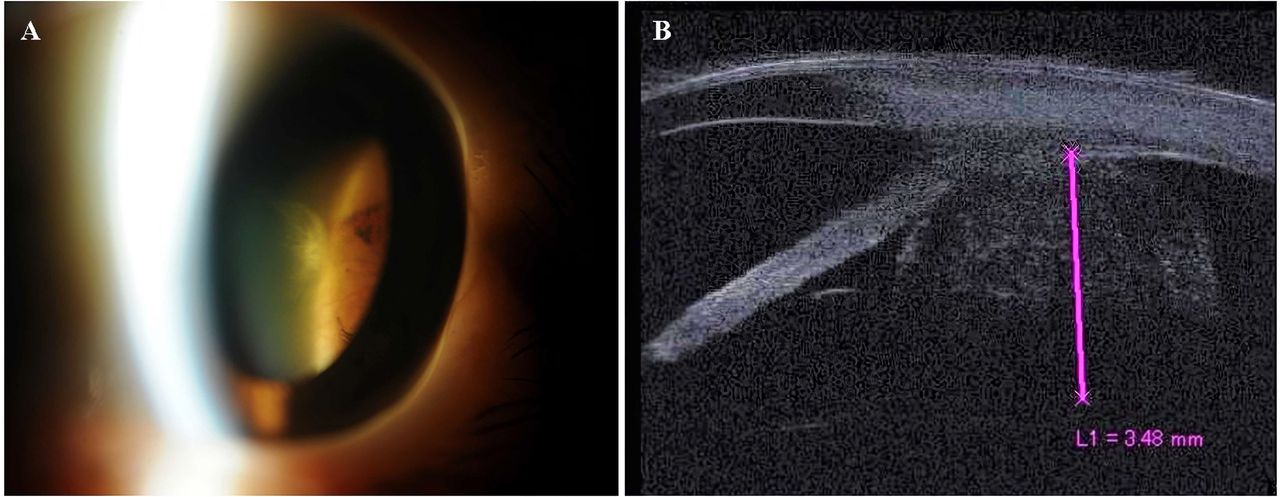
For proliferative diabetic retinopathy, vitrectomy with cataract surgery was performed on her right eye, and panretinal photocoagulation was performed in both eyes. One year later, the diabetic retinopathy in her left eye worsened, and macular haemorrhage reduced her visual acuity to 20/600 in her left eye. Additionally, the temporal ciliary tumour in her left eye enlarged (figure 1A). Ultrasound biomicroscopy revealed a 3.5–4.0 mm tumour (figure 1B). Considering the possibility of malignancy, we planned total resection of the ciliary tumour combined with vitrectomy with silicone oil tamponade and cataract surgery in the left eye.

Clinical features of ciliary granular cell tumour. (A) Slit-lamp photography. A yellowish-white solid mass is observed in the temporal periphery of the retinal and ciliary body. (B) Ultrasound biomicroscopy shows a 3.5–4.0 mm tumour.
Investigations
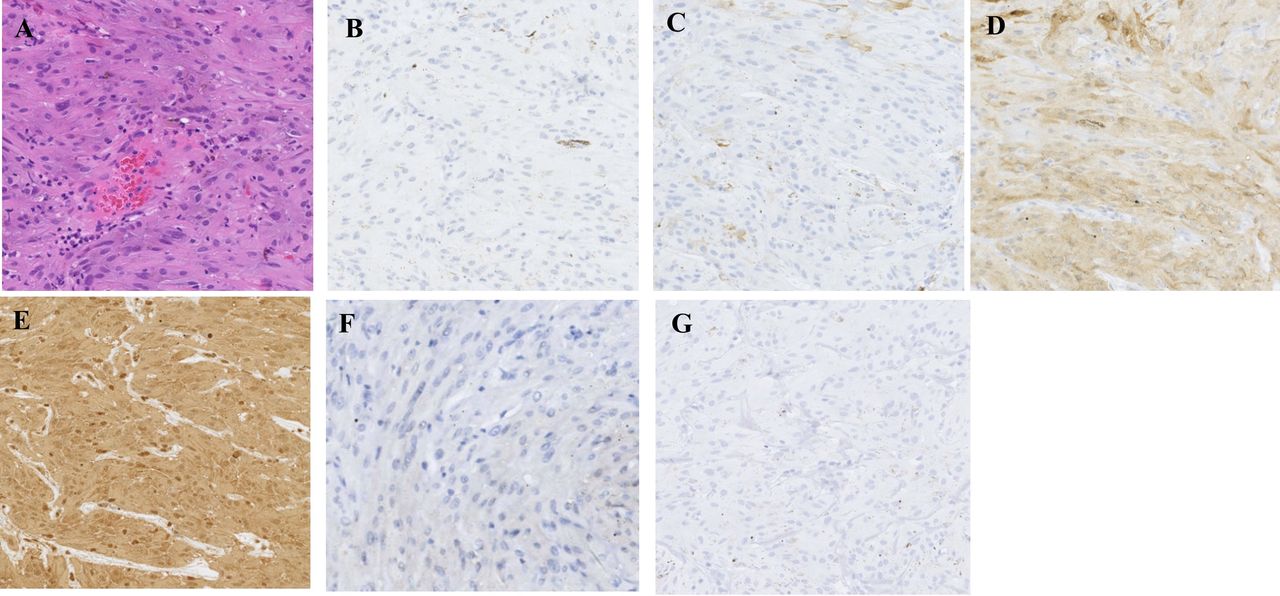
H&E staining of the excised tissue revealed (figure 2A) tumour cells with small round or oval nuclei with eosinophilic cytoplasm and some cells with spindle-shaped nuclei. These findings were suggestive of leiomyosarcoma and schwannoma, respectively. Immunohistochemical, desmin (figure 2B) and alpha smooth muscle actin staining (figure 2C) were negative, and a smooth muscle tumour was ruled out. In contrast, S-100 (figure 2D) and vimentin (figure 2E) staining were strongly positive in the cytoplasm, and the brown pigment was irregularly scattered. However, SOX-10 (figure 2F) staining was negative, suggesting it was not schwannoma. The possibility of tumour of melanocyte lineage or Schwann cell lineage was considered. Negative results of epithelial membrane antigen staining ruled out schwannoma. In addition, CD68(−), HMB45(−) (figure 2G), cytokeratin AE1/AE3 (weak) and a low Ki-index (<1%) ruled out clear cell sarcoma, melanoma and malignancy. Since spindle-shaped cells were positive for S-100 staining, the tumour was of the Schwann cell lineage. Based on these results, we diagnosed the patient with ciliary GCT.
{kind=link}
{kind=link}
Histopathological findings of ciliary granular cell tumour. (A) H&E staining (300×). The tumour cells have small round or oval nuclei with eosinophilic cytoplasm. (B–E) Immunohistochemistry staining (300×). The tumour cells are primarily negative for desmin (B), alpha smooth muscle actin (C), SOX-10 (F) and HMB45 (G), but positive for S-100 (D) and vimentin (E). Since spindle-shaped cells are positive for S-100 staining, the tumour was of the Schwann cell lineage. However, the tumour was negative for SOX-10 staining, which suggests it is not schwannoma, but a granular cell tumour.
Treatment
During surgery, phacoemulsification and intraocular lens insertion were first performed. Subsequently, the lateral rectus muscle was incised, and a semicircular half-thickness sclerotomy with a diameter of 7 mm was performed at the temporal sclera with a straight scleral knife (Alcon Grieshaber AG). After coagulation of the half-thickness scleral floor with diathermy, a semicircular full-thickness sclerectomy and partial ciliary body resection with a diameter of 5 mm were performed with a 1 mm margin on the scleral floor. The sclera and ciliary body tumour were removed together, and the vitreous body and part of the iris attached to the tumour were excised using conjunctival scissors. After the wound was closed by suturing the scleral flap with 8-0 coated VICRYL, total vitrectomy was performed. Retinal detachment around the resected tumour was minimal since panretinal photocoagulation had been previously performed. Additional retinal photocoagulation around the retinal detachment was performed, and the surgery was completed by filling the eye with silicone oil.
Outcome and follow-up
The patient’s postoperative course was uneventful, and no retinal detachment or proliferative membrane formation was observed at the resected site. Diabetic retinopathy subsided after panretinal photocoagulation. Four years postoperatively, the corrected visual acuity in the left eye was 20/100. Macular degeneration due to macular haemorrhage was observed in the left eye; however, no recurrence of the ciliary body tumour was observed on slit-lamp microscopy or ultrasound biomicroscopy.
Discussion
Tumours that develop after anticancer drug therapy are referred to as secondary neoplasms, including benign ones.
GCT, first reported by Abrikossoff and Myome in 1926,16 is a slow-growing tumour that often occurs in middle-aged adults (between 40 and 60 years of age) in the trunk, extremities, subcutaneous area and tongue and occurs more frequently in women. Abrikossoff et al also speculated that GCTs originate from neoplasms of immature striated muscle (myoblastoma). Although the histogenesis of GCT remains controversial, morphological, immunohistochemical and ultrastructural evidence suggests its neural/schwannian origin.1
Histologically, GCTs are characterised by the presence of sheets and cords of large, polygonal, round or elongated cells containing abundant eosinophilic granular cytoplasm with periodic acid–Schiff-positive eosinophilic granules.1 GCT with atypical morphology can present with spindle cell formation.1 In immunohistochemical staining, GCTs almost always express S-100 protein and vimentin.1 In contrast, cytokeratin, epithelial membrane antigen, myogenic (desmin, myogenin and smooth muscle actin) or melanic markers (Melan-A, HMB-45) are consistently negative.1
Although GCT is usually benign, 1%–2% of GCTs are malignant.16 In the periocular region, few cases of malignant GCTs, such as primary orbital tumour,17 metastatic orbital tumour,18 primary eyelid tumour19 and metastatic eyelid tumours, have been reported.20
Although no guidelines for the treatment of GCTs exist, total excision is recommended for orbital GCTs, and proton beam radiation therapy may be appropriate in case of incomplete surgical resection of benign GCT.4
Our patient developed malignant lymphoma during early childhood. Metastasis to the bone marrow occurred 2 years later, and she received a bone marrow transplant. In addition, cerebral cavernous haemangioma, primary ovarian insufficiency, indolent type 1 diabetes, growth hormone deficiency, thyroid nodules, other endocrine abnormalities and multiorgan tumours developed; however, the cause was not identified. Some of these conditions are possible complications of the bone marrow transplantation she received in late childhood. It is unclear whether ciliary GCT is associated with systemic abnormalities or bone marrow transplantation, and this should be investigated in the future.
Reports of intraocular GCTs are scarce, and to the best of our knowledge, only three cases have been reported to date.13–15 The first report was of an iris and anterior ciliary body tumour in a woman in her 20s; however, no systemic abnormalities were described in that case. The iris tumour was 1 cm in size and grew asymptomatically over 3 months. The tumour was removed via ab externo excision using a limbus-based conjunctival flap. No recurrence was observed at 1 year postoperatively.13 The second case was of a woman in her 50 s who had no systemic disease. A yellowish-white mass measuring 10 optic disc diameters that extended from the inferonasal side of the optic disc and included the optic disc was detected.14 A vasoproliferative tumour was suspected; therefore, intravitreal bevacizumab injections were administered, which were transiently effective for the suppression of exudation only, and did not reduce the mass lesion. Vitrectomy combined with tumour biopsy and silicone oil tamponade was performed. The patient was histologically diagnosed with a GCT. The tumour was completely resected, and no recurrence was observed. The third case report was of an early childhood girl with no family history of systemic diseases or tumours. She had a large, yellowish-white, elevated, subretinal mass in front of and inferior to the optic disc, with a partial inferior quadrant retinal detachment. The tumour had a distinctive border and showed no calcification on B-scan ultrasonography. A vitrectomy with lensectomy and neoplasm resection with silicone oil tamponade was performed, and histopathological examination confirmed the diagnosis of GCT. Two years after the first visit, no recurrence was noted.15 The first case report of a ciliary GCT13 is relatively similar to the current case; however, it differs from our case in that the patient did not have any systemic disease, and tumour expansion was observed within a relatively short period of approximately 3 months.
In our patient, the tumour enlarged within 1 year, and malignancy could not be ruled out. Therefore, we performed a total ab externo excision of the ciliary tumour because it was difficult to completely remove the tumour through a vitrectomy.14 15 Intraocular GCT can present in the ciliary body as a yellowish-white solid mass and should be considered as a differential diagnosis of ciliary tumours.
As the current case underwent chemotherapy for lymphoma and a bone marrow transplant during childhood, it is possible that GCTs are related to lymphoma and bone marrow transplantation. No case reports in the literature suggested the association of GCT with bone marrow transplantation. However, two case reports21 22 suggested a possible association of GCT with lymphoma. Eguchi et al reported the coexistence of primary gastric lymphoma, adenocarcinoma and GCT in a 64-year-old man.21 However, the reasons why GCT coexisted with lymphoma and adenocarcinoma were not discussed in the article. On the other hand, De Raeve et al reported a case of a 9-year-old boy who developed Hodgkin’s disease, received radiotherapy and chemotherapy and developed multiple cutaneous GCTs 3 years later.22 Although there was a possibility that GCT was a secondary neoplasm associated with Hodgkin’s disease treatment, the authors could not provide conclusive evidence on whether the association was real or coincidental.
Previous reports demonstrated that childhood cancer survivors had a higher risk of secondary neoplasms.23 24 The standardised incidence ratios for secondary malignant neoplasms in childhood cancer survivors who received chemotherapy for Hodgkin lymphoma and non-Hodgkin's lymphoma were reported as 4.0 and 2.4, respectively.24 The current case received chemotherapy for T-cell lymphoma at 2 years of age, and it is possible that GCT is a secondary neoplasm for prior lymphoma. However, to the best of our knowledge, only one case of GCT that developed after chemotherapy for lymphoma has been reported.22 If chemotherapy is indeed causally related to the onset of GCTs, more reports of GCTs as secondary neoplasms ought to have been published. Although we cannot completely deny the association of GCT with prior lymphoma, it is possible that the onset of GCT was accidental. Whether or not GCTs occur as secondary neoplasms should be investigated by accumulating more cases.
Patient’s perspective
When I was an infant, I developed malignant lymphoma and received a bone marrow transplant. Since then, I have suffered many hormonal disorders, diabetes and tumours. The tumour in my left eye was discovered by chance during an examination for diabetic retinopathy. Since the eye tumour gradually grew, and there was a possibility of malignancy, I underwent surgery to remove it. I am glad that I was able to have the surgery safely. I don't know why I have these various diseases. I hope that advances in medicine will help us understand the cause of my illness.
Learning points
Intraocular granular cell tumour (GCT) can present as a yellowish-white solid mass in the ciliary body.
Considering the very low incidence of intraocular GCT, it is difficult to diagnose GCT without a biopsy.
Approximately 1%–2% of GCTs are malignant. As it is difficult to completely remove ciliary tumours through vitrectomy, total ab externo excision is recommended in cases of rapidly enlarging tumours.
Ethics statements
Patient consent for publication
Acknowledgments
Fumihiko Toyoda and Rena Takagi have assisted in patient examination.
References
Footnotes
Twitter @Kabu
Contributors TK and YT substantially contributed to the study conceptualisation. AK and SS performed the operations and were involved in clinical follow-ups. TK and YT significantly contributed to data collection. AK and SS significantly contributed to data analysis and interpretation. TK and YT substantially contributed to the manuscript drafting. All authors critically reviewed and revised the manuscript draft and approved the final version for submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.