Article Text

Abstract
A previously well man in his 50s returned to the UK after a trip to the Mediterranean. The day after returning he developed malaise, fevers, rigors and severe headache. He was hospitalised with sepsis, multiorgan involvement, a maculopapular rash and an eschar on each hip. Serology was positive for Rickettsia spp (spotted fever group) with a rise in titre from 1:64 to 1:1024 eight days later. Blood and tissue PCR were also positive for Rickettsia spp. He had cardiac, pulmonary, renal, ocular and neurological involvement. He completed a 14-day course of doxycycline and recovered well. This is a case of likely Mediterranean spotted fever (MSF) caused by Rickettsia conorii, which is endemic to the Mediterranean basin. We highlight the need for awareness and early treatment to prevent severe complications. This case is also the first to describe Purtscher-like retinopathy in the context of likely MSF.
- Travel medicine
- Tropical medicine (infectious disease)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Mediterranean spotted fever (MSF) is an uncommon disease in returning travellers to the UK. Most patients have a short, self-limiting illness without the use of antibiotics, but untreated disease can lead to severe complications and may even be fatal. Worldwide rates of rickettsial diseases have been increasing, presumed secondary to climate change and increased contact between humans, animals and vectors that transmit rickettsiae. It is important that clinicians consider rickettsial diseases as one of many possible causes of fever and rash in returned travellers from endemic areas such as the Mediterranean basin. Empiric doxycycline in this scenario can be life-saving.
Case presentation
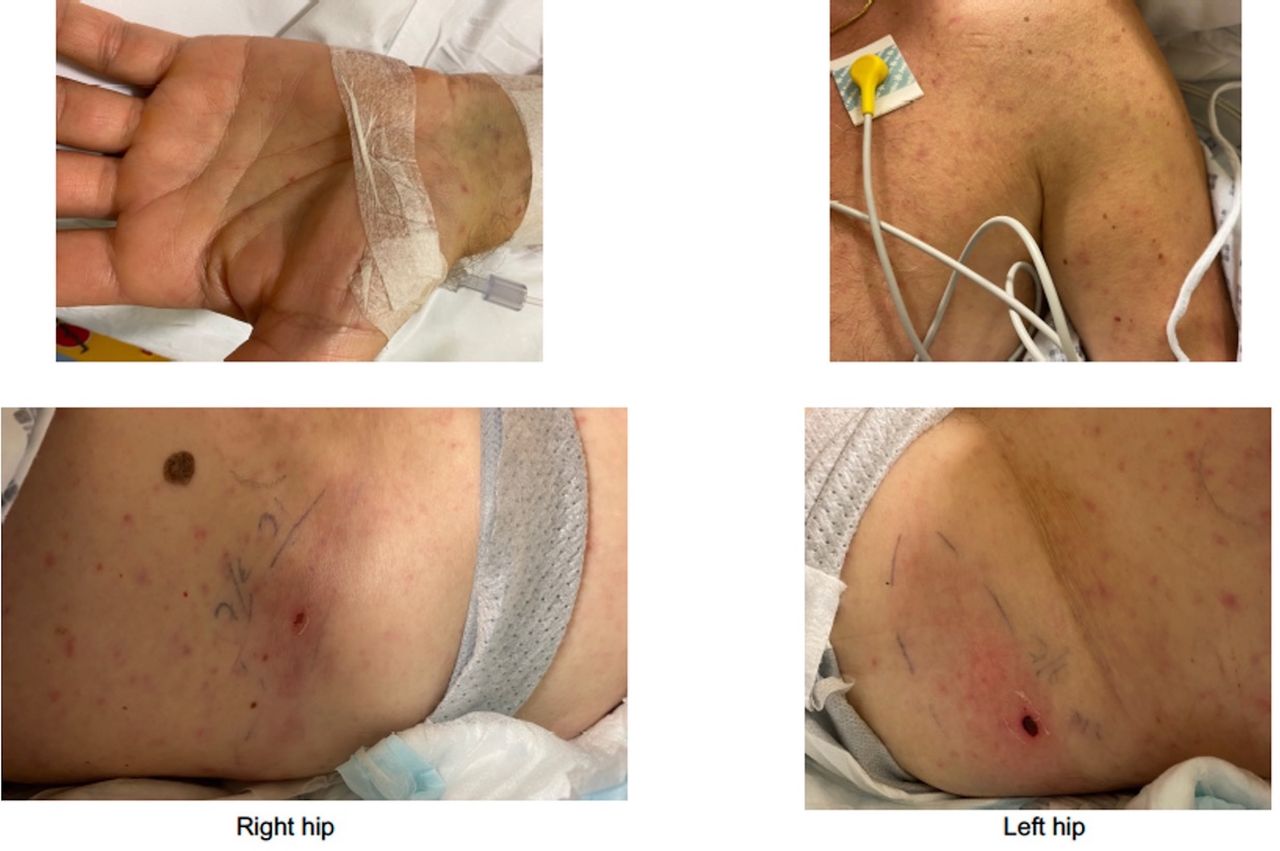
A previously well man in his 50s returned to the UK after a week-long trip to a rural area of the Mediterranean basin. During this trip in late spring, he spent several days clearing an overgrown garden. The day after returning he developed malaise, fevers, rigors and severe headache. On day 3 of illness, he was reviewed via telehealth in primary care and given flucloxacillin for a possible spider bite. On day 4, he developed shortness of breath, then on day 5, he developed a rash which was seen by a paramedic and the patient was advised to take antihistamines. On day 7 of illness, the patient’s wife noticed that the rash had spread and the patient’s general clinical condition had deteriorated significantly. He was seen in primary care again that day and taken by ambulance to his local hospital. On arrival to the emergency department, the patient was febrile with a temperature of 38°C–39°C. He was in fast atrial fibrillation (AF) with a rate of 115 beats per minute and was hypotensive with a blood pressure of 85/60 mm Hg despite 6 L of fluid resuscitation. He was noted to have a diffuse, erythematous, non-blanching maculopapular rash involving the anterior torso, limbs and palms (figure 1). The rash was asymptomatic and spared the face, back and soles of the feet. The patient was not sure which part of the body the rash had started on. The lesions on the anterior torso and limbs were around 0.5–1 cm in diameter and the lesions on the palms were <0.5 cm in diameter. There was also a brown eschar on each hip just lateral to the inguinal creases (figure 1). The left eschar was more prominent, with surrounding erythema of approximately 17×7 cm compared with the right side (erythema approximately 10×3 cm). The patient also had bilateral non-purulent conjunctivitis but denied symptoms such as eye pain or vision loss. His heart sounds were dual with no murmurs and crackles were noted at both lung bases. His abdomen was full but there was no organomegaly palpable. He had a mild hand tremor at rest.

Examples of the rash and eschars on each hip.
At the time of admission, the patient could not recall any animal contact, bites or stings while he was overseas. He drank bottled water and did not swim in any bodies of fresh water. He owned cats in the UK, which were all healthy. The patient was not taking any regular medications and was fully immunised as a child.
Investigations
Initial blood tests showed a mild anaemia (haemoglobin 120 g/L), thrombocytopaenia (platelets 88×109/L), a significant inflammatory response (ferritin 11 621 ng/mL, C reactive protein 217 mg/L, D-dimer 9166 μg/L) and mild hepatitis (alanine aminotransferase or ALT 172 U/L) with a normal bilirubin of 18 umol/L. Creatine kinase (CK) and lactate dehydrogenase (LDH) were both elevated (CK 259 U/L, normal range 30–200 U/L and LDH 721 U/L, normal range 125–243 U/L). A blood film did not show malaria parasites and a malaria dual parasite test (Plasmodium falciparum, Plasmodium knowlesi and Plasmodium ovale) was also negative.
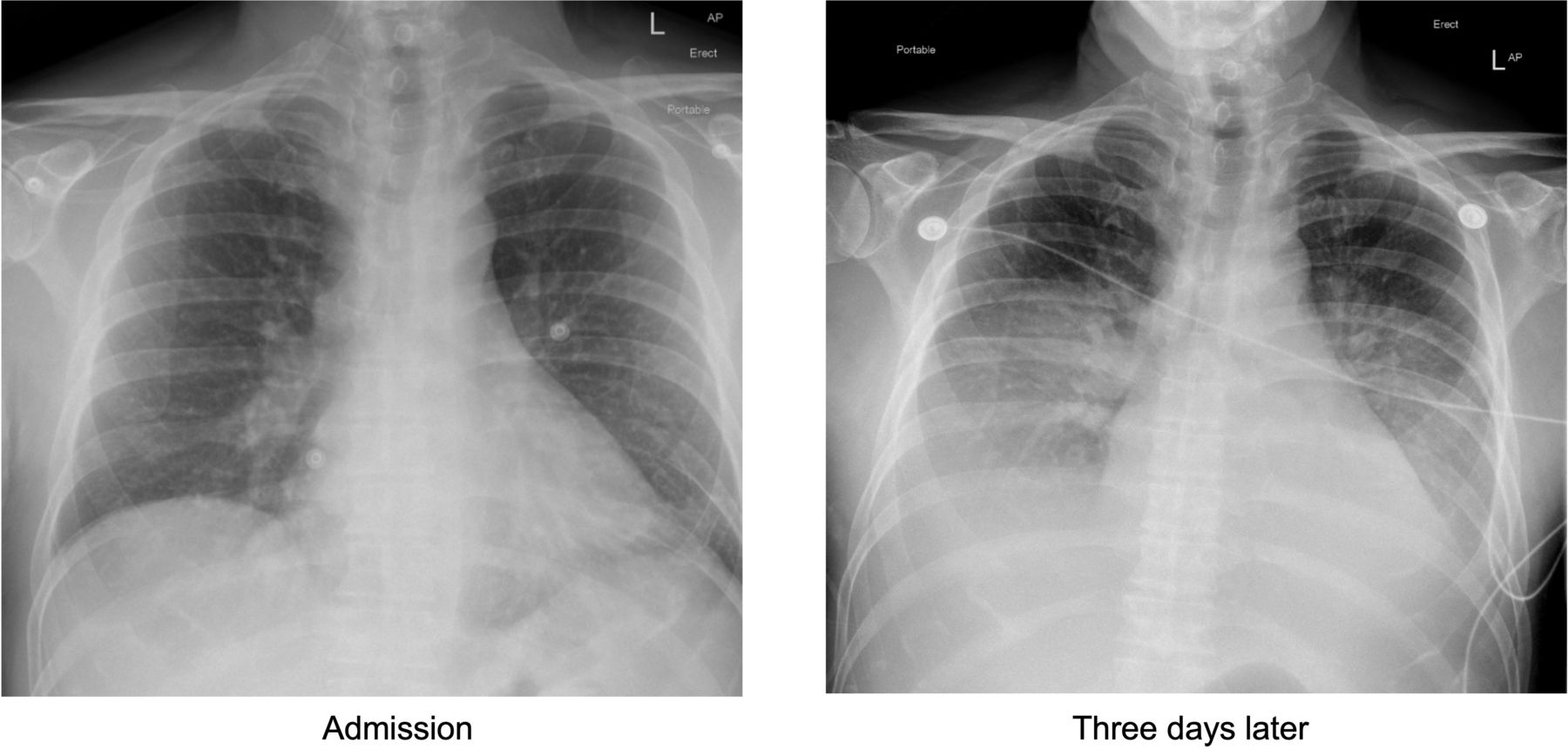
Initial chest X-ray (CXR) showed left lower lobe changes consistent with bronchopneumonia (figure 2). A CT pulmonary angiogram showed small bilateral pleural effusions with adjacent collapse or consolidation and cardiomegaly. CT abdomen/pelvis was essentially normal apart from small volume ascites; notably, there was no hepatosplenomegaly, lymphadenopathy or collection. An echocardiogram was also unremarkable.

Admission chest X-ray (CXR) showing minor bronchial wall thickening in the left lower lobe which could be due to infection or inflammation. CXR 3 days later showing bilateral moderate size pleural effusions and upper lobe diversion.
The eschars on the patient’s hips became black on day two of admission. Repeat CXR 3 days after admission showed fluid overload with bilateral pleural effusions and upper lobe diversion (figure 2). Troponin was mildly elevated with a peak of 63.4 ng/L (normal range <34.2 ng/L). ECG showed no evidence of myocarditis.
The patient was discussed with local infectious diseases teams as well as tropical disease experts from the Imported Fever Service at the Rare and Imported Pathogens Laboratory in Porton Down and a blood sample was sent for testing. Blood Rickettsia GltA real-time PCR based on a published assay by Stenos et al1 was positive for Rickettsia spp. Samples were extracted using the Qiagen QIAamp DNA mini kit and the PCR was performed using the Invitrogen Superscript III Platinum One-step Quantitative RT-PCR kit on the Roche LightCycler480.
Based on this positive PCR result, the clinical findings and epidemiology, a presumptive diagnosis of MSF was made (figure 3). Serology was subsequently positive for Rickettsia spp (spotted fever group) with a rise in titre from 1:64 to 1:1024 eight days later. Tissue PCR from the left hip eschar was also positive for Rickettsia spp. Whole-genome sequencing confirmation of rickettsial species is awaited and has been delayed due to sequencing pressures from the COVID-19 pandemic.
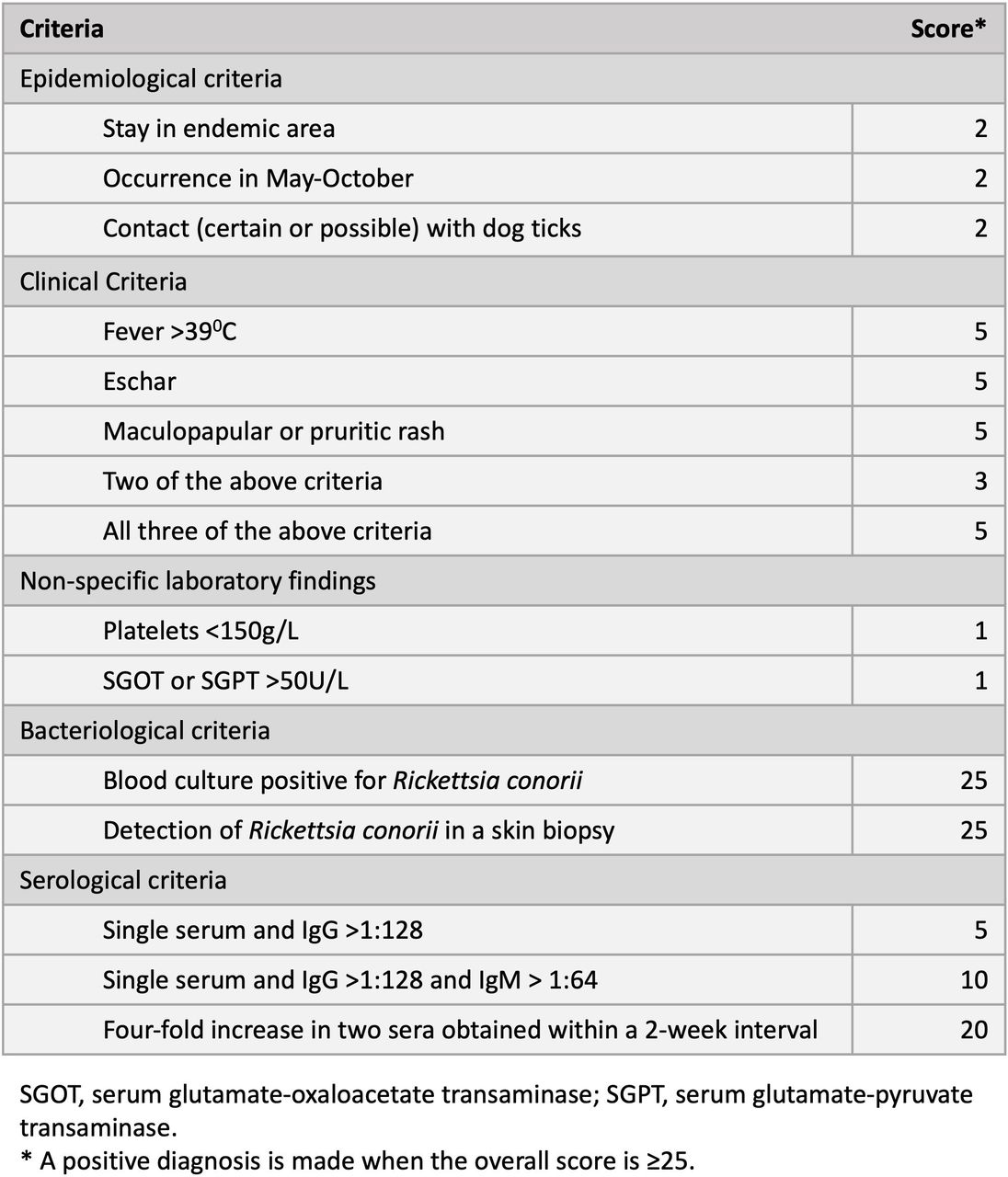
Diagnostic criteria for Mediterranean spotted fever (MSF). Reprinted from Clinical Microbiology and Infection, vol 10 edition 12, Brouqui P, Bacellar F, Baranton G, Birtles R, Bjoërsdorff a, Blanco J, et al, Guidelines for the diagnosis of tick-borne bacterial diseases in Europe, Pages 1108–32, Copyright 2004, with permission from Elsevier.
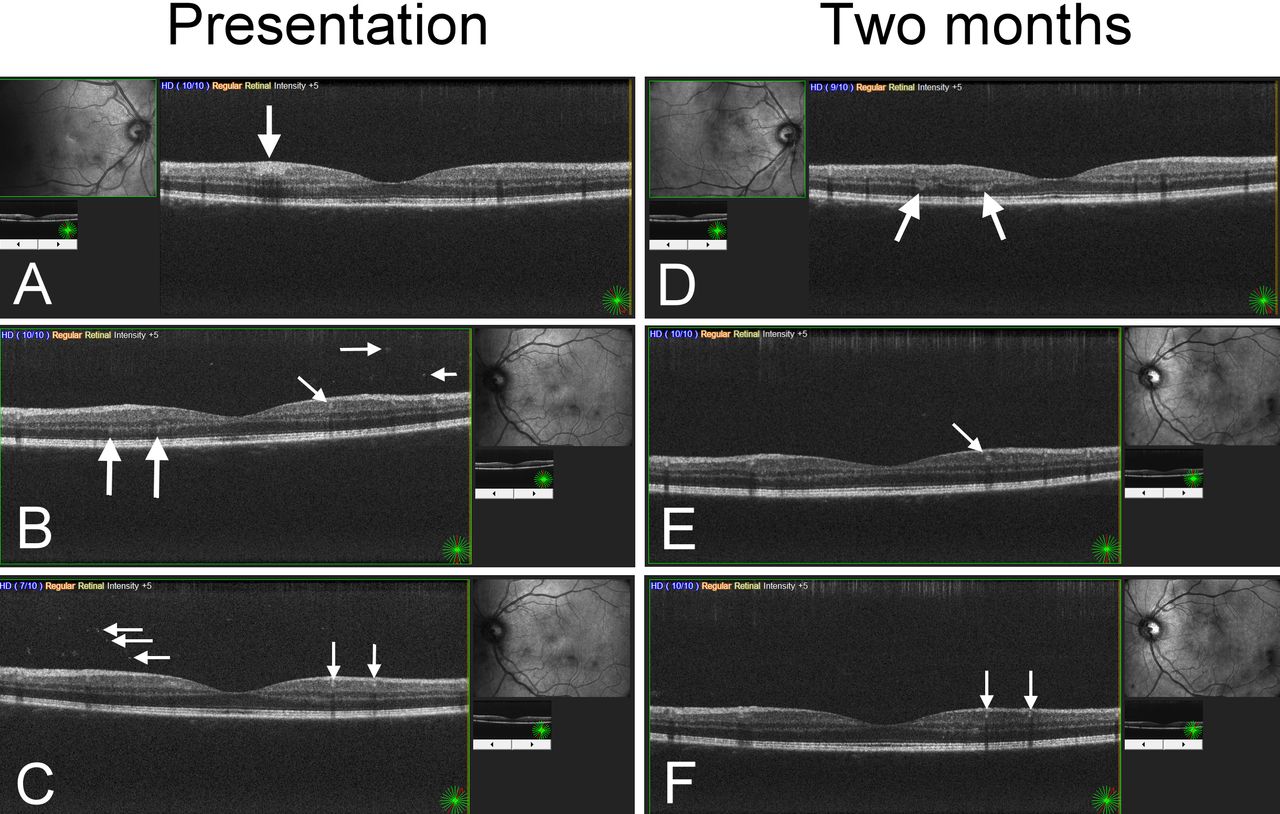
An ophthalmology consultation was sought on day 6 of admission due to the presence of bilateral conjunctivitis, even though the patient remained asymptomatic. Recumbent ophthalmic examination was performed using an indirect ophthalmoscope and hand-held slit lamp as the patient was too weak to be moved to the ophthalmology department. A mild papillary conjunctivitis with ciliary injection was present in both eyes, but there was no detectable anterior uveitis or vitritis. Multiple large cotton wool spots respecting vessel borders (Purtscher flecken) were seen on funduscopy in retinal zones A, B and C, as well as occasional haemorrhages in zone A in both eyes. The patient was examined again 5 days later and fundus images were captured. By this time, the number of Purtscher flecken had reduced dramatically in the right eye and almost disappeared from the left, although involvement of zone C could still be seen (figure 4). Optical coherence tomography (OCT) was also done, which showed abundant vitreous cellular activity and vitreous debris (figure 5B,C, horizontal arrows) in addition to hyper-reflective dots within the inner nuclear, inner plexiform and outer plexiform layers of the retina in both eyes (figure 5A–C, vertical and oblique arrows). There was also a solitary infiltrate within the inner portion of the inner plexiform layer probably extending into the ganglion cell layer (figure 5A, vertical arrow).

Retinal pictures (retinal zones reprinted from Br J Ophthalmol, Vol 91 edition 11, Agrawal A and McKibbin M, Purtscher’s retinopathy: epidemiology, clinical features and outcome, Pages 1145–6, Copyright 2007, with permission from BMJ.).

Optical coherence tomography.
Differential diagnosis
Many possible differential diagnoses were considered including bacterial sepsis, SARS-CoV-2 infection, HIV seroconversion illness, secondary syphilis and mycoplasma. Several other diseases endemic to the Mediterranean basin may have caused a similar presentation including West Nile virus, Crimean-Congo haemorrhagic fever (CCHF) and murine typhus. Other tickborne diseases such as borreliosis, tularaemia and ehrlichiosis were considered a possibility, as well as leptospirosis given the liver dysfunction and conjunctivitis. Measles was included in the differential list although the patient reported receiving all childhood vaccinations. Malaria was considered but ruled out. Dengue, chikungunya and leishmania were considered unlikely. The presence of Purtscher flecken was intriguing but the list of conditions causing Purtscher-like retinopathy was too vast to narrow the differential. Autoimmune disease was discussed with the rheumatology team but was felt to be unlikely. The haematology team were also consulted but felt that haemophagocytic lymphohistiocytosis (HLH) complicating infection was unlikely because the patient had normal triglycerides of 2.7 mmol/L, normal fibrinogen of 3.5 g/L and no splenomegaly.
Treatment
The patient was started on empiric doxycycline on arrival to hospital. Given the severity of his symptoms, multiorgan involvement and likelihood of malabsorption with severe sepsis, he was started on intravenous doxycycline 200 mg two times per day. He continued this for 3 days and was then switched to the standard oral dose of 100 mg two times per day. He completed a 14-day course of antibiotics.
The patient’s fever resolved 36 hours after starting doxycycline. He was in the intensive care unit (ICU) for 5 days and required cardiovascular support for just over 24 hours. His fast AF was treated with a loading dose of digoxin and amiodarone, after which he reverted back to and remained in normal sinus rhythm. Respiratory support (as much as 70 L/min of 0.7 FiO2 high-flow nasal oxygen) was needed for the entirety of his stay in ICU. He was then discharged to the ward where he required low flow nasal oxygen until just prior to discharge on day nine of admission (day 16 of illness).
Outcome and follow-up
The patient was well on face-to-face clinical review 2 weeks after discharge. He reported a significant amount of weight loss, ongoing mild hand tremor at rest and some mild subjective hearing impairment. His blood tests showed improvement in his inflammatory markers with a ferritin of 2701 ng/mL, normal renal function and improvement in his liver function with an ALT of 194 U/L (peak ALT 230 U/L).
Ophthalmology review 2 months later confirmed almost complete resolution of ocular signs. OCT at that time showed resolution of vitreous cellular activity and debris in both eyes (figure 5D–F) with reduced but ongoing hyper-reflective dots (figure 5E, F, arrows). The infiltrate in the right eye appeared to have become segmented and distributed into several patches of hyper-reflectivity in the same location (figure 5D, arrows).
Four months after discharge, the patient reported being completely recovered and free of any lasting symptoms.
Discussion
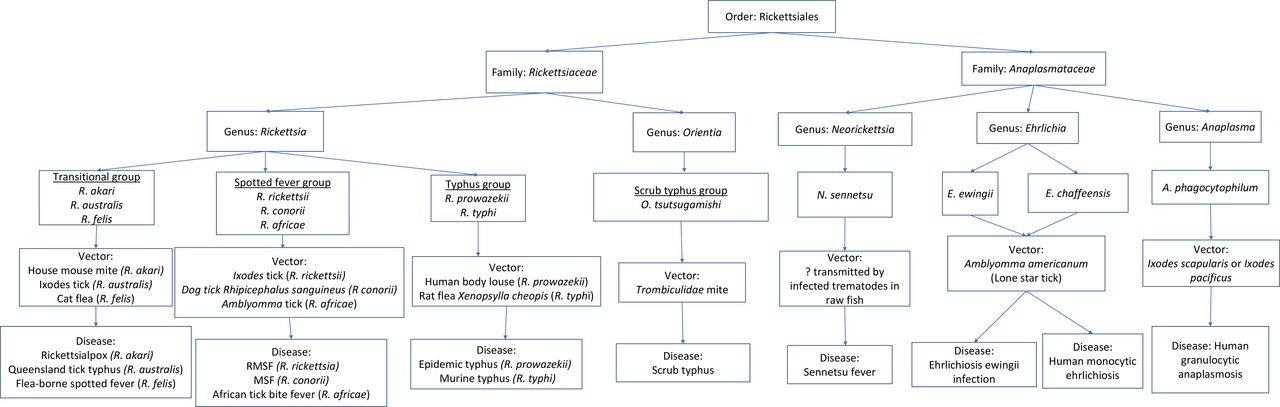
Human rickettsial diseases are caused by bacteria of different genera including, but not limited to, Rickettsia, Orientia, Neorickettsia, Ehrlichia and Anaplasma (figure 6). Almost all rickettsial diseases are transmitted by an arthropod vector. MSF is part of the spotted fever group which includes Rocky Mountain spotted fever. Rickettsial diseases can cause a spectrum of disease from self-limiting, mild symptoms to severe illness and can be difficult to differentiate on clinical grounds alone. Some important differential diagnoses such as CCHF, West Nile virus and leptospirosis can also present with similar clinical symptoms to MSF, therefore expert laboratory diagnosis is invaluable.2 However, positive serology may be misleading due to cross-reactivity with other rickettsial species such as Rickettsia typhi,3 the causative agent of murine typhus, which can make diagnosis challenging given that both diseases are endemic to the Mediterranean basin.4
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Human rickettsial diseases.
MSF was first described in Tunisia in 19105 and is endemic to the Middle East, India and Africa as well as the Mediterranean basin. It is the most common zoonosis in Mediterranean countries such as Portugal6 and classically occurs during the summer months. Reports of MSF incidence in Mediterranean countries have decreased in recent years.7 8 However, the worldwide incidence of rickettsial diseases is increasing due to increasing human travel and environmental degradation9 associated with climate change, leading to increased contact with vectors and humans or animal reservoirs.
The causative organism of MSF is the obligate intracellular gram-negative bacterium Rickettsia conorii. The vector is the brown dog tick Rhipicephalus sanguineus (sensu lato). The animal reservoir includes dogs, small mammals and ticks.5 Ticks can be either vector or host of R. conorii and humans are an incidental host. Only about 10% of patients notice a tick bite.6 A black eschar (tache noire) at the site of the tick bite is present in 60%–72% of cases,2 10 usually on the trunk.6 There is typically only a single eschar, however, multiple eschars have been described,11 which could be due to multiple tick bites over several days’ exposure in the case of our patient. The incubation period of MSF is around 7 days, following which patients commonly present with sudden onset of high fever and influenza-like symptoms, particularly headache and myalgia. Around 7 days after the onset of the fever, the patient usually develops a classic maculopapular spotted rash which involves the trunk, limbs, palms and soles but spares the face, as seen in our patient.
Although MSF usually causes a mild, self-limiting disease, complications can occur either in the acute or convalescent phase. In the acute phase, disseminated symptoms occur as a result of vascular endothelial cell invasion by R. conorii.5 9 12 This leads to a systemic vasculitis, which can cause renal failure, myocarditis, pneumonia, anicteric hepatitis and encephalitis.12 Gastrointestinal bleeding and rhabdomyolysis13 can also occur. MSF can trigger the onset of HLH.14 15 HLH was an initial concern in our patient given the high ferritin, however, he did not progress to develop a clinical or biochemical syndrome consistent with HLH. Complications in the convalescent phase of MSF are thought to be mostly secondary to immune-mediated mechanisms and are primarily neurological, including sensorineural hearing loss,9 aseptic meningitis, meningoencephalitis, myelitis, polyradiculoneuritis and facial paralysis. Ocular complications can also occur, classically multifocal retinitis affecting the posterior pole with macular serous detachment and vitritis.16
Our patient had evidence of ocular inflammation and was diagnosed with Purtscher-like retinopathy which, to our knowledge, has not been previously described in conjunction with MSF. Purtscher retinopathy is an occlusive microangiopathy associated with trauma and usually causes loss of vision.17 Characteristic retinal findings include cotton-wool spots, intraretinal haemorrhages and areas of intraretinal whitening called Purtscher flecken.17 In the absence of a history of trauma, as in our patient, the retinal findings are called Purtscher-like retinopathy. Purtscher-like retinopathy has been described in association with conditions including pancreatitis, renal failure, autoimmune disease, infections such as acute hepatitis C18 and is often associated with multiorgan failure and a high mortality rate.19 Purtscher flecken involving retinal zone C are a very rare finding, as these lesions most commonly involve zone A and less often zone B.19 Therefore, further reports of rickettsial illness are needed to establish whether retinal zone C involvement is a characteristic of rickettsial disease in general, or MSF in particular. However, infectious triggers other than hepatitis C are not well described and it is possible that the presence of Purtscher-like retinopathy in this case reflects severe systemic disease rather than a defined pathological process associated with rickettsial diseases.
Tetracyclines are the treatment of choice for rickettsial diseases.2 5 20 MSF is most commonly treated with doxycycline 100 mg two times per day for 7–14 days, depending on clinical severity.5 Alternatives to doxycycline include chloramphenicol and macrolides such as azithromycin.10 20 Given the unknown central nervous system (CNS) penetration of doxycycline, dosing in CNS rickettsial disease can be as high as 200 mg two times per day for the first 72 hours.21 Our patient was initially prescribed intravenous doxycycline given likely gastrointestinal malabsorption secondary to sepsis-induced ileus. Once he was able to tolerate oral intake, he was converted to oral dosing.
There are no vaccines available for rickettsial diseases and antibiotic prophylaxis is not recommended.20 Prevention of disease involves regular self-checks, avoidance of ticks and tick habitats, wearing barrier clothing and using insecticides.5 Mortality of MSF in countries such as Portugal is around 3.6%,6 but can be as high as 60% without treatment.20 Mortality rates and disease severity tend to be worse in adults than children.22 Our patient had a very good clinical outcome despite a late presentation with severe rickettsial disease with multiorgan involvement.
Patient’s perspective
In late spring I took a trip to the Mediterranean. I was bitten by an insect in the long grass but dismissed it because this often happens. Within a few days of my return home, I started to feel unwell. The bite became red and black. I spoke to the GP and sent them a picture and they prescribed antibiotics. Over the next couple of days, I felt worse despite the antibiotics so went to see the GP. I had not realised how sick I was but the GP was fantastic. He took one look at me and immediately referred me to A&E and then organised an ambulance to take me there.
On arrival at the hospital, I could not have received better care and attention. Initially, they could not diagnose what was wrong with me. They ran extensive tests including blood tests, ECGs and a chest X-ray. While trying to diagnose the problem they gave me a cocktail of treatments and monitored me carefully. I was transferred to ICU where I received 1:1 care 24 hours of the day.
The staff were amazing. They were compassionate, kind and supportive. Not only to me but also to my wife, keeping her up to date on my condition and enabling her to visit me or speak to me when she could not be there. I cannot remember everything that happened, or unfortunately, everyone that looked after me, while in ICU. But I do remember how caring everyone was. One doctor even held my hand when I was at my lowest, that act of kindness was very reassuring and I will never forget that gesture. They looked after me and made me feel that nothing was too much trouble even though I felt a burden.
With the help of expert colleagues they were able to diagnose me with Mediterranean Spotted Fever from a tick bite and gave me the treatment I needed.
After 5 days in ICU and a further 4 days on a ward, I was allowed home. I am still recovering but should get back to normal thanks to the fantastic, professional and caring service I received from the NHS.
If you ever get bitten by an insect, either here or abroad, do not dismiss it. Insect bites can cause as many problems as spider or snake bites which you may take more seriously. If you feel unwell or the bite starts to get red make sure you seek medical advice. If after starting antibiotics you feel no better or worse go back and see your GP.
While it is very easy to complain I felt compelled to put pen to paper and say what absolutely fantastic treatment I received both from my GP and everybody at the hospital. The NHS is a wonderful institution with some amazing people that deserve to be recognised. No one wants to be critically ill but it is reassuring to know that we have some outstanding individuals that are dedicated to making you well again and look after you when you need it. I would not be here today without the wonderful medical team and I cannot thank them enough.
Learning points
Mediterranean spotted fever (MSF) is a common zoonosis in Mediterranean countries, and a small number of cases occur in returning travellers to the UK each year, mostly during the summer months.
Tickborne diseases are increasing worldwide due to increased travel and climate change. They can be difficult to differentiate on clinical grounds and prompt accurate diagnostics are essential.
While most patients have a self-limiting illness, MSF can cause severe disease with multiorgan involvement in some cases. Our patient had severe rickettsial disease with pulmonary, cardiac, ocular, hepatic and neurological involvement. Confirmation of MSF is awaited.
This is the first published report of Purtscher-like retinopathy occurring in a patient with probable MSF.
Early empiric treatment with doxycycline when differential diagnoses include rickettsial diseases may prevent the development of severe illness.
Ethics statements
Patient consent for publication
Acknowledgments
Thank you to the staff at UKHSA RIPL Porton Down for the expert advice and support, particularly Tim Brooks and Tommy Rampling.
References
Footnotes
Twitter @aahmado
Contributors KD wrote the initial draft and subsequent drafts. AA provided details and images related to ophthalmology. CEW, LOD, JF and KS provided suggestions and corrections.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.