Article Text

Statistics from Altmetric.com
Description
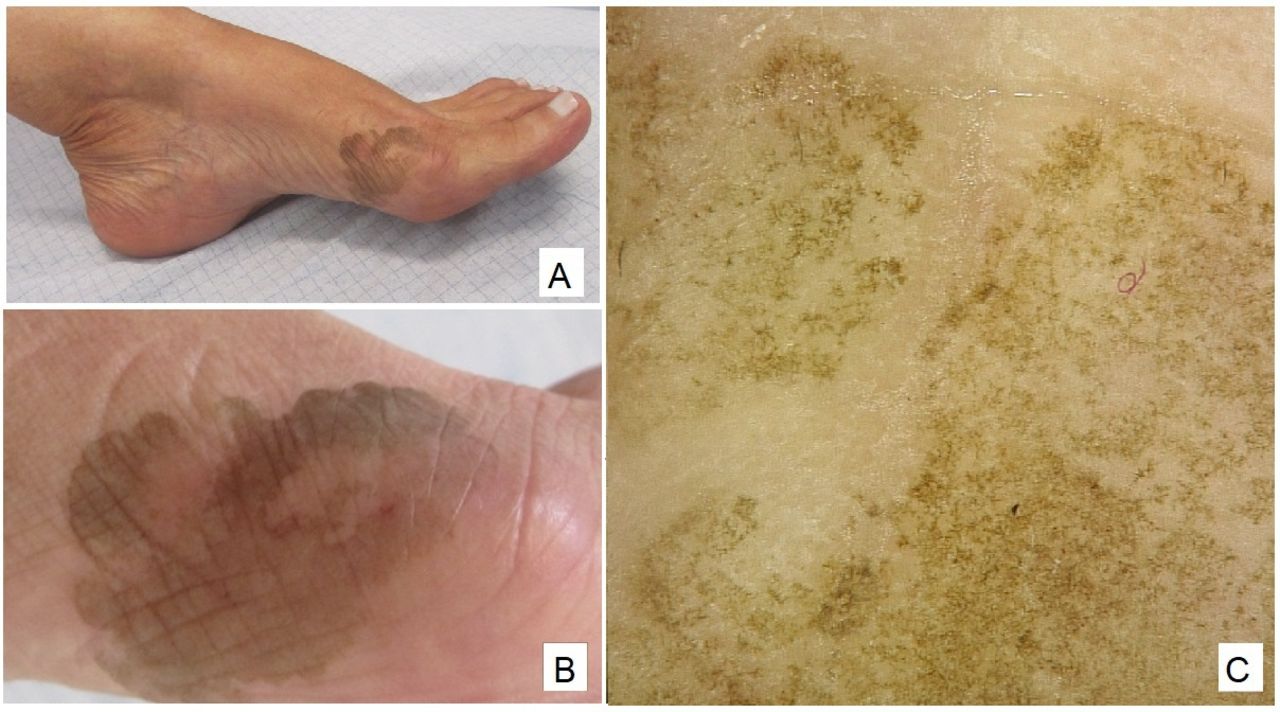
A woman in her 60s, skin phototype III, presented to the dermatology clinic for a pigmented lesion on her left foot that had been growing slowly for the last 5 years. Clinical examination disclosed, over the internal border of the first left metatarsophalangeal joint, a well-demarcated, non-desquamative, irregularly pigmented dark patch with a diameter of 6 cm (figure 1A,B).
{kind=link}
(A) Brown patch with irregular contours over the first left metatarsophalangeal joint; (B) higher-magnification image showing a light brown lesion with irregular contours; (C) dermoscopy of the lesion (×10).
Dermoscopy (figure 1C) showed superficial fine, wispy pigmented spicules, that did not respect the dermatoglyphic lines, corresponding to pigmented hyphae in the stratum corneum. A direct mycological examination disclosed irregular, branching, septate dematiaceous hyphae and yeast-like cells with spores, and a superficial shave biopsy showed multiple hyphae on the corneal layer, confirming the clinical suspicion of tinea nigra. Treatment with topical cetoconazol resulted in complete resolution.
Tinea nigra is clinically characterised by a gradually enlarging, irregularly pigmented macula on the palms and soles, which can be confused with melanocytic lesions. It is a superficial phaeohyphomycosis that occurs mainly in tropical or subtropical areas and is caused by the mould Hortae werneckii.1 2 Dermoscopy, the clinical presentation, and direct examination with potassium hydroxide (KOH) confirm the diagnosis. Dermoscopy is a useful clinical adjuntive tool in differentiating tinea nigra from a melanocytic lesion, and may avoid unnecessary invasive procedures, such as biopsies.
Learning points
Tinea nigra is a superficial mycosis caused by Hortae werneckii, that may be confused with melanocytic lesions, such as acral melanoma.
Although H. werneckii usually occurs in tropical or subtropical areas, with globalisation, these infections have increasingly been reported in Europe.
Dermoscopy helps to confirm this diagnosis, potentially avoiding invasive procedures.
Ethics statements
Patient consent for publication
Footnotes
Contributors AGP: study conception and planning; critical literature review; preparation and writing of the manuscript. RS: critical literature review, manuscript critical review. AM-C: study conception and planning; approval of the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.