Article Text

Statistics from Altmetric.com
Description
A man in his 80s was transferred from a regional to a metropolitan centre with a gastric outlet obstruction secondary to a large aortic sac that developed following a previous abdominal aortic endovascular aneurysm repair (EVAR). The functionally independent patient initially presented with abdominal pain, distention and bilious vomiting preceded by several days of intermittent nausea. He had a history of an elective EVAR 7 years previously to treat an abdominal aortic aneurysm (AAA). It was known that the aortic sac had been gradually increasing in size over many years (from 7.5 cm in 2015 to 10.7 cm in 2021) with no demonstrable acute leak on serial multiphase imaging, including contrast-enhanced duplex ultrasound. An elective graft explantation with open repair had been discussed; however, no definite plans were made due to the patient’s multiple comorbidities, hostile abdomen from previous multiple abdominal surgeries and advanced age.
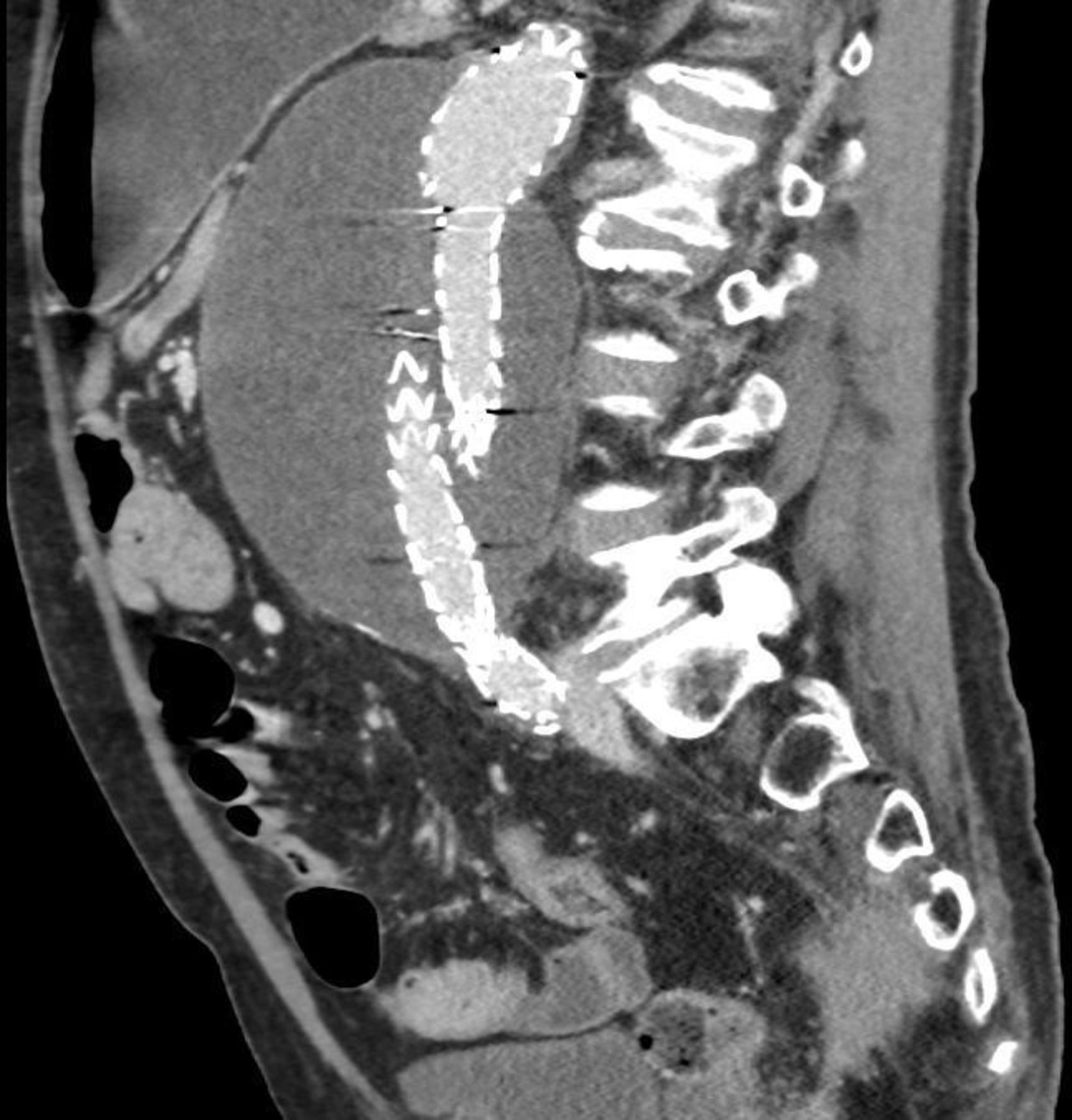
A multiphase CT scan was performed. It demonstrated an aortic sac 11 cm in diameter with EVAR in situ (figure 1). The third part of the duodenum was compressed between the large aortic sac and the superior mesenteric artery (figure 2). The delayed phase imaging showed no acute endoleak (figure 3), favouring endotension as the mechanism of aortic sac expansion. Endotension or type V ‘endoleak’ is a poorly understood phenomenon describing aortic sac expansion in the absence of detectable endoleak.1

Coronal CT image demonstrating EVAR and an aortic sac.
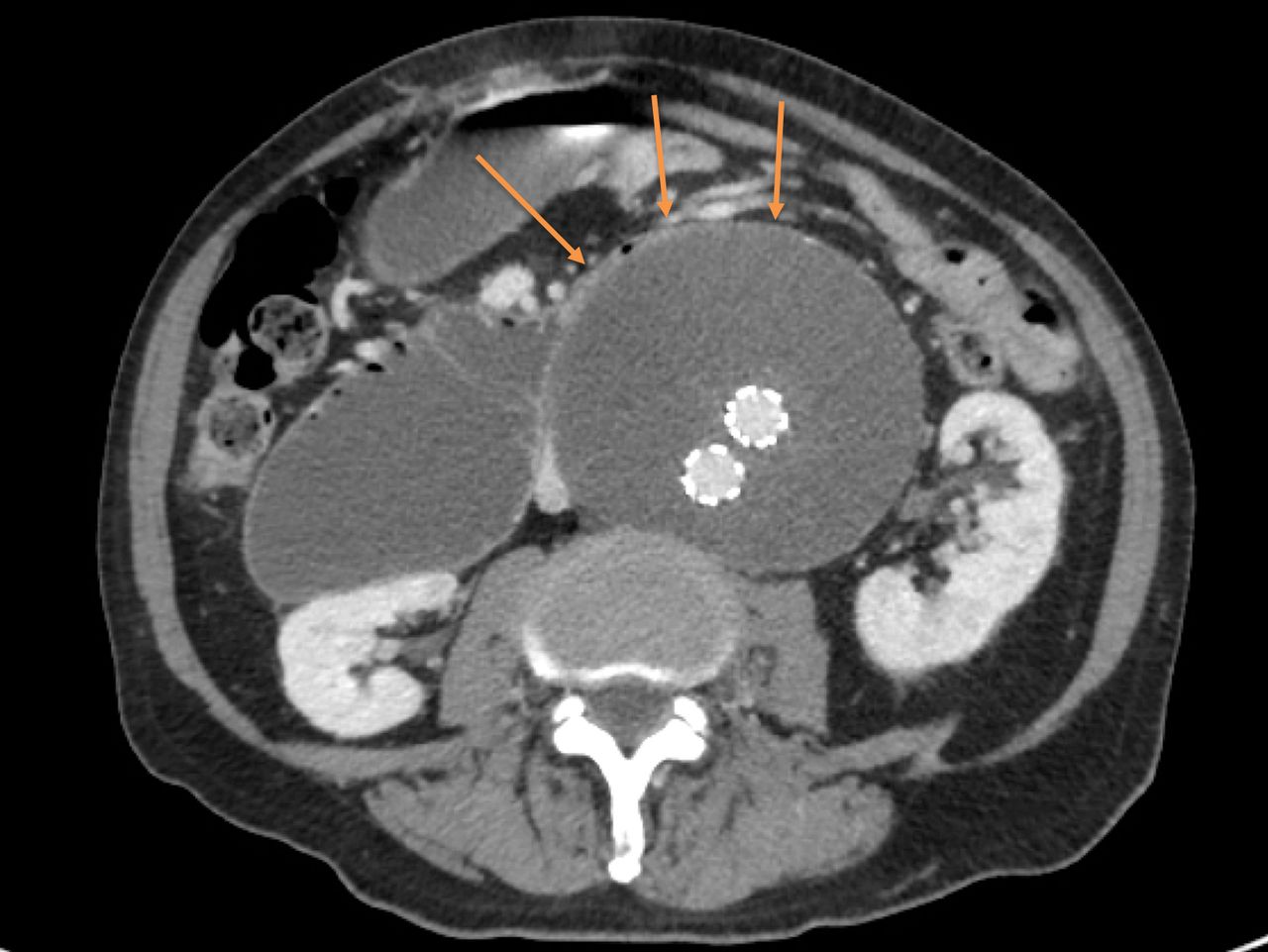
Axial CT image demonstrating obstruction of the duodenum at D3 between the aortic sac and Superior mesenteric artery (SMA).
{kind=link}
{kind=link}
{kind=link}
Sagittal delayed multiphase CT image showing no endoleak.
A nasogastric (NG) tube was placed for decompression, and adequate resuscitation and maintenance were implemented. Electrolyte imbalances were corrected, and total parenteral nutrition was instituted. Interdisciplinary consultations were made between the vascular, general and upper gastrointestinal surgical teams. The options discussed were gastrojejunal bypass to relieve the gastric outlet obstruction versus aortic surgery to explant the failed EVAR. The patient was definitively managed with explantation of the EVAR and placement of a bifurcated silver-impregnated graft, as we could not safely remove the proximal portion of the graft, which was cut short and left in situ. No leak was found intraoperatively. The patient required admission to the intensive care unit (ICU) postoperatively and returned to the ICU with hospital-acquired pneumonia. The patient was discharged home via a peripheral rehabilitation hospital.
Duodenal obstruction secondary to AAA, also known as an aortoduodenal syndrome, was first described by Osler in 1905 and remains a rare cause of gastrointestinal obstruction.2 It is well recognised that the initial management of this presentation should consist of decompression with an NG tube, electrolyte optimisation and nutritional optimisation before consideration of surgical management.3 4 Management of aortoduodenal syndrome with gastrojejunostomy procedure to bypass the obstruction in the setting of previous EVAR has been described in the literature.5 To the author’s knowledge, this case report is the first to describe management with EVAR explantation. As visualised on CT, this patient’s extreme aortic sac dilatation influenced this management decision. By proceeding with the EVAR explantation, the source of gastric outlet obstruction was removed, and the risk of future aortic rupture was eliminated. Despite the significant risks, definitive management with EVAR explantation enabled this patient to return to an independent lifestyle.
Learning points
Aortoduodenal syndrome is a rare cause of small bowel obstruction.
CT visualisation of the endovascular aneurysm repair (EVAR), aortic sac and obstruction point inform multidisciplinary discussions and aid risk stratification and decision making around definitive management.
This case demonstrates that high-risk EVAR explantation surgery is a viable management option for aortoduodenal syndrome, even in patients with multiple comorbidities.
Ethics statements
Patient consent for publication
Footnotes
Contributors JC: writing—original draft. MGN: conceptualisation, project administration, writing—review and editing. OAO: supervision, writing—review and editing. RR: supervision, writing—review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.