Article Text

Statistics from Altmetric.com
Description
A young adult man presented to the otolaryngology department having progressive hearing loss in his right ear for 3 months after a febrile illness. There were no associated reports of ear pain, ear discharge, vertigo or trauma. On otoscopic examination, there was a minimal retraction of the tympanic membranes on either side. The rest of the clinical examination was unremarkable.
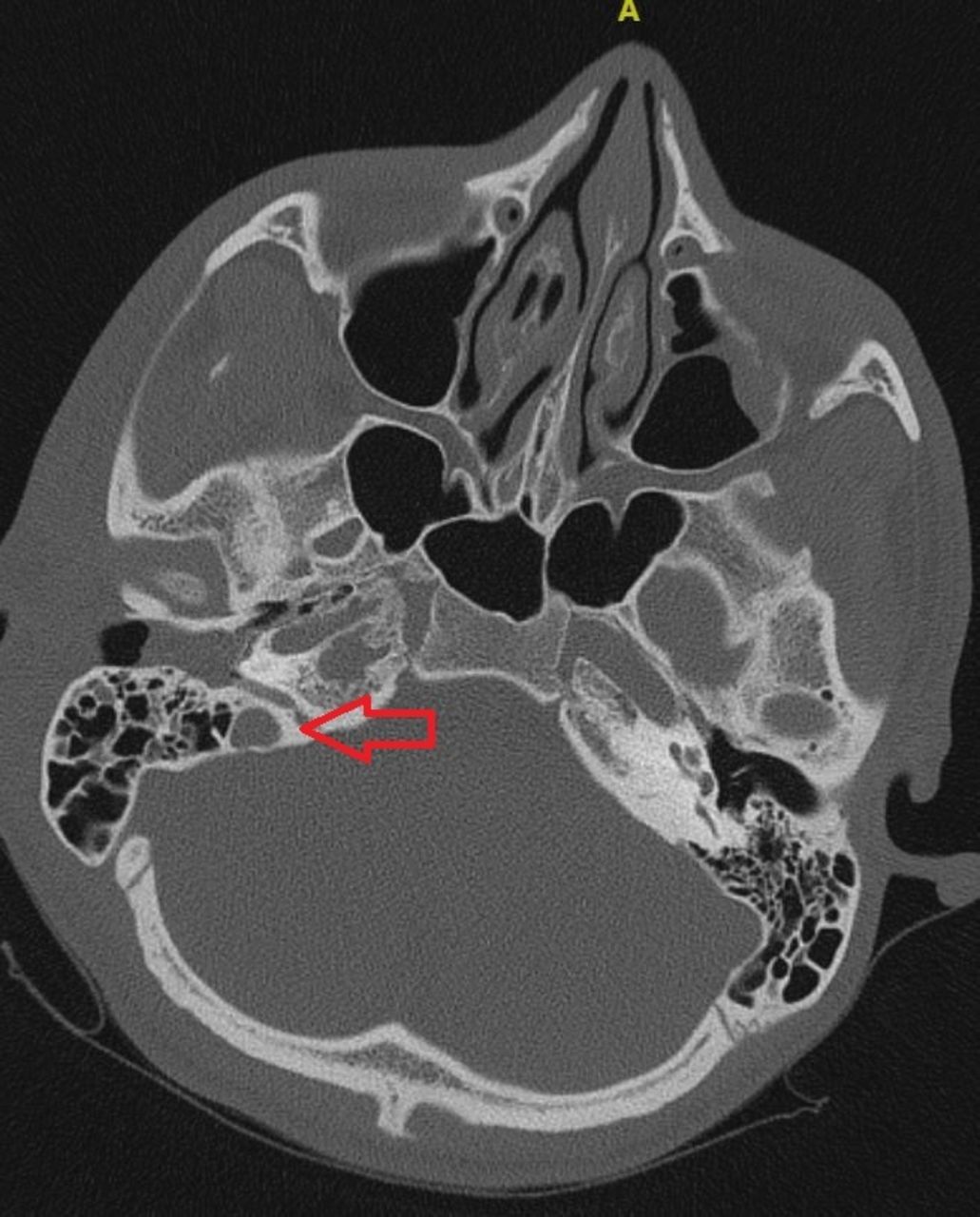
A pure tone audiogram revealed a profound sensorineural hearing loss of 90 dB on the right, with a normal hearing threshold on the left. Tympanometry was unremarkable. A high-resolution CT of the temporal bones showed an expansile smooth-walled lesion of size 7 mm × 10 mm in the right petrous apex, with overlying cortical thinning (figures 1 and 2). No other abnormality was noted in the middle ear or inner ear. The patient subsequently underwent an MRI of the brain with contrast, which confirmed the presence of a well-defined cystic lesion of the right petrous apex. It was hyperintense on both T1 and T2, suggesting a cholesterol granuloma or a cholesteatoma (figure 3). The only possible surgical approach to the lesion was a cell tract, beginning in the hypotympanum, inferior to the basal turn of the cochlea. The patient was counselled regarding surgical drainage of the cyst but the irreversibility of his hearing loss.

Preoperative HRCT temporal bone (axial section). The yellow asterisk depicts the cavity in the right petrous apex. HRCT, high-resolution CT.

Preoperative HRCT temporal bone (coronal section). The yellow asterisk depicts the granuloma in the petrous apex. The red arrow shows the precarious infracochlear route to the petrous apex. HRCT, high-resolution CT.

Preoperative MRI (T2 axial section). The yellow arrow depicts the hyperintense petrous apex contents.
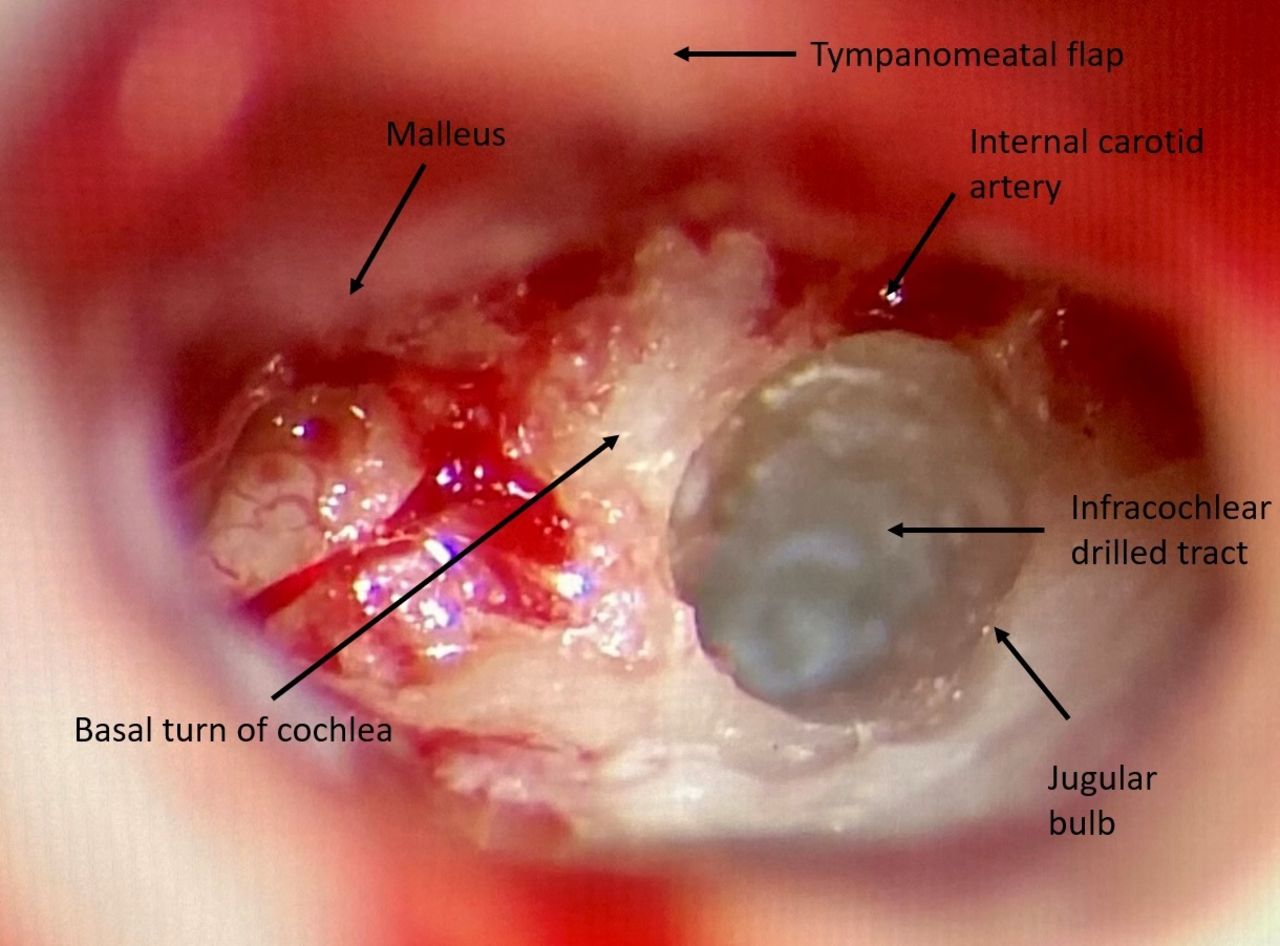
The patient underwent a posterior tympanotomy and drilling was done along the infralabyrinthine cell tracts to the petrous apex. Drilling for the infralabyrinthine approach was done in a roughly triangular space inferior to the basal turn of the cochlea, posterior to the internal carotid artery and anterior to the jugular bulb (figure 4). No well-defined tract was visualised, and the solid bone was drilled to a depth of 12 mm when a dome of a cyst-like structure appeared in the view. When this cyst-like structure was opened, there was a gush of cerebrospinal fluid. A misaligned trajectory of the drilling appeared to have led to the posterior fossa dura and not the petrous apex. The track was closed with fat harvested from the abdominal wall and reinforced with temporalis fascia and fibrin glue. A postoperative CT scan (figure 5) showed the trajectory of the surgical tract was more posteriorly angled by around thirty degrees, leading to the posterior fossa dura and not the petrous apex. The postoperative course was uneventful, and the patient is planned for a repeat procedure after about 6 months when the tract will hopefully be fibrosed.

Intraoperative photograph obtained during the exposure of the infracochlear tract. The various landmarks are depicted.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Postoperative HRCT temporal bone (axial section). The red arrow depicts the tract created surgically for the drainage of the petrous apex lesion. HRCT, high-resolution CT.
Cholesterol granulomas encompass the most frequent destructive lesion of the petrous apex.1 Cholesterol granulomas form when the aeration of the petrous apex is hindered, thus creating a vacuum into which blood is drawn, causing foreign body giant cell reaction to cholesterol deposits, with fibrosis.2 They are ten times more common than cholesteatomas and forty times more common than petrous apex mucoceles.3 They are usually clinically silent but can bring about local mass effects, resulting in headaches, hearing loss, diplopia and vertigo.4 Five approaches were traditionally employed to gain surgical access to the petrous apex: middle cranial fossa, translabyrinthine, transotic, infracochlear and infralabyrinthine.
In patients with serviceable hearing, lesions encroaching the posterior wall of the sphenoid sinus can be approached via the transsphenoidal route also.5 The infralabyrinthine approach via the transmastoid path is the most preferred means to drain these lesions. The infracochlear approach is preferred for lesions below the internal auditory canal and preserves hearing by bypassing the auditory apparatus. A narrow route exists to the petrous apex, with surgical tracts limited mainly by a high jugular bulb.6
Although the translabyrinthine approach offers direct access to the petrous apex in an unserviceable ear,7 we employed the infralabyrinthine approach for the patient. In the present case, the lack of infra labyrinthine cells or a tract, the small size of the lesion, a sizeable distance of over a centimetre between the middle ear and the lesion and the non-availability of intraoperative navigation contributed to us missing the lesion and leading us to the posterior fossa dura and eventually cerebrospinal Fluid (CSF) leak. The narrow corridor of approach and the critical boundaries such as the jugular bulb and the carotid artery predisposes to complications such as CSF leak, haemorrhage and complete loss of serviceable hearing. Facial palsy is an expected complication; however, seizures and meningitis are also theoretically possible.
Based on the location of the petrous apex cyst, alternative routes of endoscopic endonasal approaches have been advocated such as the transclival and the infrapetrous approach, but are contraindicated in cases where the cyst is hidden behind the internal carotid artery (ICA).8 However, if the lesion is proximal to the internal auditory canal and there is loss of hearing, the transmastoid approaches are preferable. In cases of patients with a non-hearing ear, drainage of the cholesterol granuloma should not be compromised with respect to exposure if the translabyrinthine approach is being adopted. This approach provides the most direct route and usually does not require entry into the intracranial compartment.
Ideally, a surgeon should follow the cell tracts anteromedially along the long axis of the temporal bone towards the petrous apex, aided by intraoperative navigation. The cyst should be emptied completely, irrigated extensively and then stented into the mastoid cavity using the largest fitting silicone catheter to avoid recurrences. Double barrel stenting has been described when two tracts are drilled into the cavity. Plugging of the tract with a pedicled muscle flap obviates the possibility of stent blockage, migration and granulations, which may otherwise predispose to recurrence.
Intraoperative mishaps can be prevented by the judicious use of surgical navigation systems and intraoperative nerve monitoring. Considerable experience is paramount for undertaking drainage of these lesions. Adequate practice on cadaveric temporal bones helps in developing and honing the skills necessary for undertaking such a procedure. Clinically silent lesions can be observed and surgery is considered only when indicated due to hearing loss or cranial nerve impairments. A thorough review of preoperative radiographs should be undertaken and good hypotympanic pneumatisation should be ensured to obtain an adequate cell tract for the infralabyrinthine approach. A high-jugular bulb precludes this approach. Good marsupialisation and adequate stenting with or without cavity obliteration gives good results, however, recurrences are common and the patient must be made aware of the possibility.
Patient’s perspective
Initially, I was worried about the hearing loss in my right ear. I was told it might not improve after surgery. I was told about a cyst near my ear, which caused this. My surgery was undertaken; however, my hearing didn’t improve though the doctors tried their best.
Learning points
The infralabyrinthine route offers the most direct route to the petrous apex from the middle ear.
The trajectory of drilling must be along the long access of the petrous bone; drilling too anteriorly or posteriorly can damage vital structures.
A CSF leak complicating the infralabyrinthine approach can be effectively dealt with using fat and fascia.
Ethics statements
Patient consent for publication
Footnotes
Contributors SC: data collection, drafting the article, patient follow-up. AA: operated on the patient, revised the manuscript for important intellectual content and approved the final version. SPR: contributed to the literature search and obtained patient consent. LKP: contributed to the literature review, revised the manuscript for important intellectual content and approved the final version of the manuscript to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.