Article Text

Statistics from Altmetric.com
Description
A man in his 70s presented with a 3-year history of dropped head syndrome (DHS). He had been diagnosed with nasal natural killer/T cell lymphoma 7 years ago, cured with concurrent chemoradiotherapy with dexamethasone, etoposide, ifosfamide, carboplatin and local radiation of 50 Gy in 25 fractions.
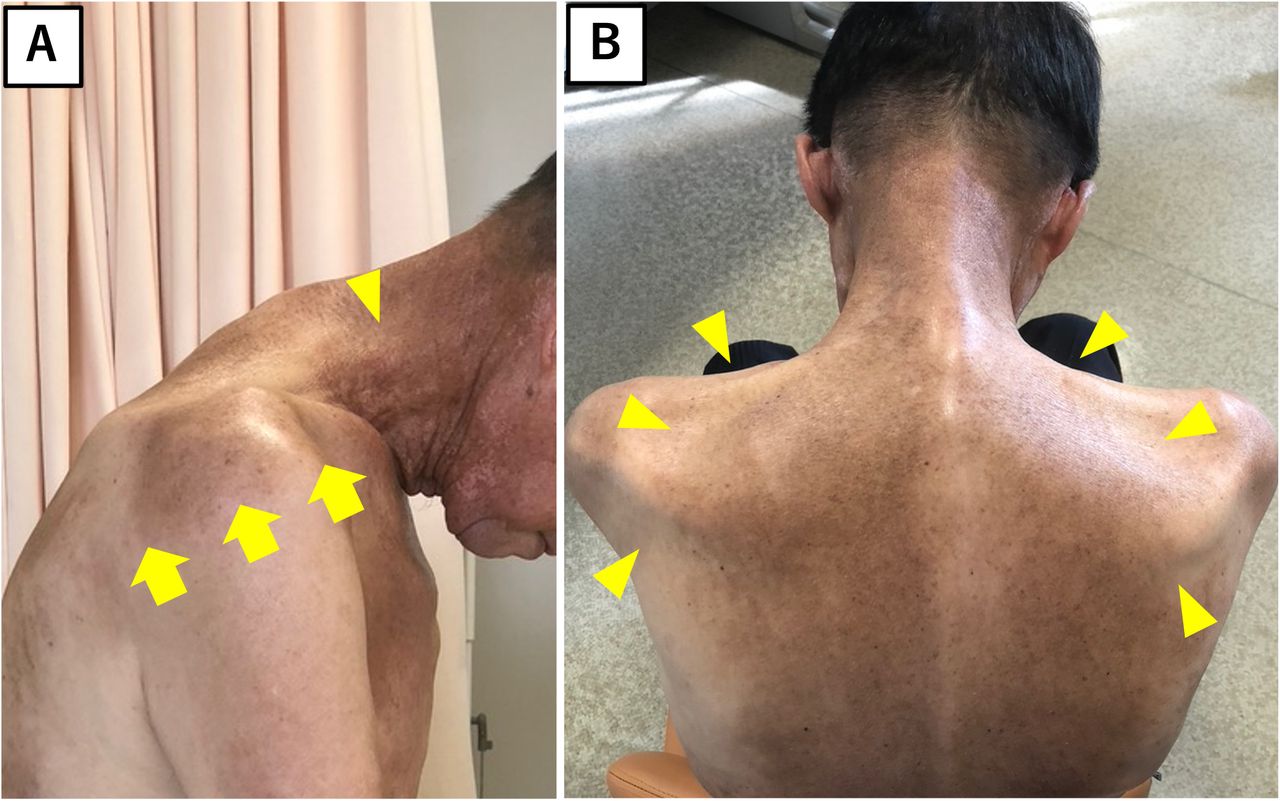
A remarkable drop in the patient’s head was observed (figure 1A). Neurological examination revealed the weakness of the neck flexor and extensor muscles (manual muscle testing, 2/5 each). Symmetrical muscle atrophy also appeared in the neck and shoulder muscles, including the sternocleidomastoid, trapezius, supraspinatus and infraspinatus (figure 1, arrowheads). Tongue atrophy was also observed, and salivary secretion and pharyngeal sensation were decreased. Furthermore, skin pigmentation with well-demarcated borders was observed on the neck and shoulders (figure 1A, arrows).

Lateral view of the patient. Anterior flexion of the neck (dropped head) is remarkable. The sternocleidomastoid muscle is atrophied (arrowhead). The skin of the upper chest, shoulders, neck and back shows symmetric pigmentation with a well-demarcated border (arrows) (A). Posterior view of the patient. The trapezius, supraspinatus and infraspinatus show symmetric atrophy (arrowheads). The overlying skin of the shoulders and back is diffusely pigmented (B).
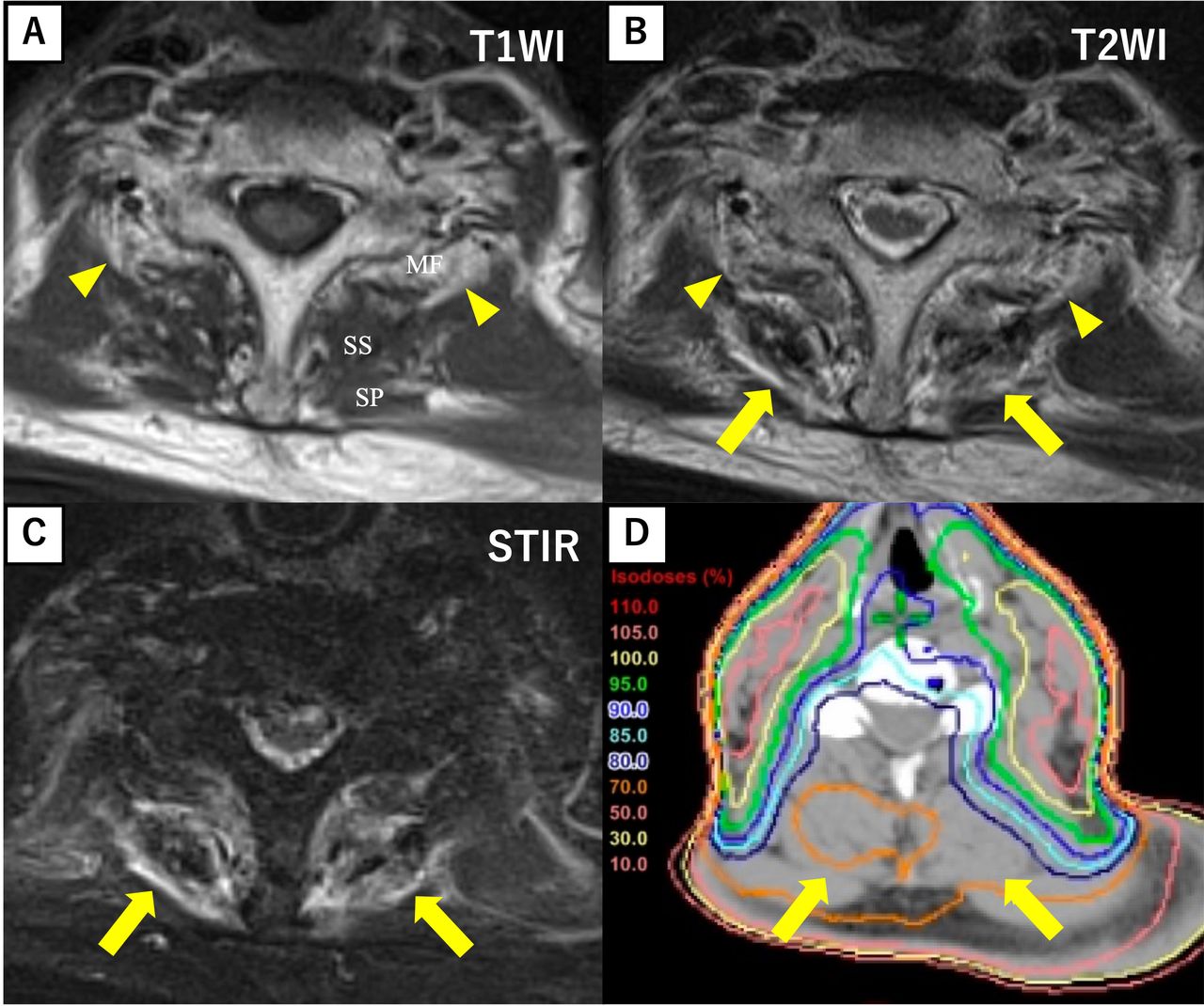
No abnormalities were detected in nerve conduction studies nor blood tests for creatine kinase, aldolase and autoantibodies. Dopamine transporter test results were also normal. Electromyography (EMG) showed short-duration, low-amplitude motor unit potentials with reduced recruitment patterns in the paraspinal muscles at the C5 spinal level. Cervical MRI revealed muscle atrophy and fatty changes (figure 2A,B, arrowheads), and the posterior cervical paraspinal muscles showed high signal intensity in T2-weighted and short tau (time to inversion) inversion recovery (STIR) images (figure 2B,C, arrows).
{kind=link}
{kind=link}
Axial view of MRI of the neck at the C6/7 spinal level. A T1-weighted image (T1WI) shows hyperintensity in the multifidus muscle adjacent to the laminas, indicating fatty degeneration (arrowheads) (A). A T2-weighted image (T2WI) shows hyperintensity in the posterior paraspinal muscles, including the semispinalis and splenius (arrows), in addition to the hyperintensity in the multifidus muscles seen in the T1WI (arrowheads) (B). A short tau inversion recovery (STIR) image demonstrates hyperintensity in the posterior paraspinal muscles, including the semispinalis and splenius (arrows) (C). The radiation dose distribution map of the C4 spinal level is shown. The numbers listed on the left reflect the different proportions of the total dose of 50 Gy, depending on each encircling line. Posterior cervical paraspinal muscles (arrows) received only up to a 70% dose, which means they received only 35 Gy (D). MF, multifidus; SS, semispinalis; SP, splenius.
Because the STIR high signal intensity was limited to the posterior neck muscles, we considered isolated neck extensor myopathy (INEM).1–3 However, based on extensive muscle atrophy and radiation-associated findings, the patient was diagnosed with DHS due to chemoradiotherapy. Unfortunately, he died from aspiration pneumonia a year later.
DHS is a condition characterised by severe kyphotic deformity of the cervicothoracic spine and can have a variety of causes, including INEM, Parkinson’s disease, myasthenia gravis, amyotrophic lateral sclerosis, inflammatory myopathy and radiation-induced myopathy.4 5 In our case, the diagnosis of DHS due to chemoradiotherapy was made based on muscle atrophy, pigmentation, EMG findings and secretory reduction in the irradiated area.
Radiation-induced DHS is a rare, delayed complication of high-dose mantle-field radiation therapy6–9; therefore, >50 Gy to the neck extensor muscles is not recommended.10 The diagnosis is challenging because of its late onset after irradiation and non-specific findings including muscle biopsy.11 12 Sometimes EMG shows a myopathic morphology with a neuropathic pattern.13 14 Given that the posterior neck received only 35 Gy of the total dose (figure 2D, arrows), concurrent chemotherapy may have enhanced radiation-induced adverse effects, as previously reported.15
The high STIR signal intensity observed in the posterior neck muscles was inconsistent with the radiation dose distribution map. The STIR change may result from secondary inflammatory changes caused by chronic stress due to a dropped head rather than direct damage from chemoradiotherapy.
In conclusion, this case highlights the importance of a thorough physical examination for the diagnosis of radiation-induced DHS. In addition, STIR high signal intensity in the cervical paraspinal muscles, as reported in cases of INEM, may be observed in radiation-induced DHS. Furthermore, DHS occurs long years after moderate-dose irradiation of neck extensor muscles in combination with chemotherapy.
Learning points
Radiation-induced dropped head syndrome (DHS) can be supported by radiation-associated findings based on detailed physical examination.
Radiation-induced DHS can show short tau inversion recovery high signal intensity limited to the cervical paraspinal muscles.
DHS occurs with a long-latency time even after moderate-dose irradiation in combination with chemotherapy.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors RI was actively involved in the patient’s care and diagnosis and made a major contribution to drafting the manuscript. MS was actively involved in the patient’s care and diagnosis and revised the manuscript. MY was involved in the patient’s follow-up after the radiation therapy and edited the manuscript. RT supervised the patient care and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.