Article Text

Abstract
Sinonasal teratocarcinosarcomas (SNTCSs) are rare and aggressive malignant tumours with histological features of the three embryonic layers. They have an elevated local recurrence rate, risk of metastasis and mortality. Moreover, the therapeutic options are limited, and optimal management is not yet clear. As fewer than 150 cases have been reported, therapeutic strategies remain a clinical challenge. Here, we discuss a case of a large SNTCS successfully treated with surgical resection followed by concurrent chemotherapy and radiation. Despite the significant size of the tumour and the inferred high recurrence risk, the patient has had no recurrence over the past 45 months. Although the optimal treatment of SNTCS is not clearly outlined, the very limited data suggests that a multidisciplinary approach with surgery, radiation and chemotherapy is the best option for patients.
- Oncology
- Head and neck cancer
- Chemotherapy
- Radiotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Sinonasal teratocarcinosarcomas (SNTCSs) are rare high-grade tumours with histological features of carcinomas, sarcomas and teratomas. They remain poorly understood, as they have been historically misclassified, and less than 150 cases have been reported in the medical literature. They are more common in male than female patients (7:1), and the average age of presentation is about 54.7 years.1
These neoplasms affect the sinonasal tract, mainly the nasal cavity and paranasal sinuses; in fact, roughly half of the patients have ethmoidal sinus involvement, one-quarter involving the maxillary sinus.1 Due to the very aggressive nature of these tumours, intracranial extension is also frequently seen. The mortality rate has been reported to be nearly 60% within 3 years, with a mean survival time of fewer than 2 years.1
Histologically, these tumours have features of malignant teratomas, carcinomas and sarcomas that include glandular and ductal structures, squamous epithelium that has fetal-like clear cell appearance and contains abundant glycogen, and a variety of mesenchymal elements, which are typically chondrosarcoma, osteosarcoma, rhabdomyosarcoma or immature neuroepithelial elements, sometimes with rosettes and neurofibrillar matrix.2
The immunohistochemical nature of SNTCSs shows positive staining for cytokeratin and epithelial membrane antigen for epithelial components; CD99, neuron-specific enolase, chromogranin, glial fibrillar acidic protein, S-100 protein, synaptophysin target neuroepithelial elements and rhabdomyosarcomatous areas stain for desmin, vimentin and myogenin.3
Here, we discuss a challenging SNTCS case treated with a multidisciplinary approach.
Case presentation
A man in his 50s sought medical attention at an emergency department due to difficulty breathing through the nose.
A CT scan and subsequent MRI revealed a sizeable soft tissue mass in the nasopharynx. The lesion measured 1.6×6.3×4.6 cm3. It arose from the medial wall of the lateral wall of the nose extending into the ostiomeatal complex, the left frontal recess and the sphenoethmoidal recess. There was also associated fullness and expansion of the pterygopalatine fossa (figure 1 A–C).

(A) T1- weighted gadolinium MRI images showing large 1.6×6.3×4.6 cm3 in the left nasal cavity and left maxillary sinus (white arrow). (B) T1- weighted gadolinium MRI images showing large 1.6×6.3×4.6 cm3 in the left nasal cavity and left maxillary sinus (white arrow). (C) T1- weighted gadolinium MRI images showing large 1.6×6.3×4.6 cm3 in the left nasal cavity and left maxillary sinus (white arrow).
The patient was in a good state of health. He had a history of benign goitre, hypertension and benign prostatic hyperplasia.
Investigations
Imaging
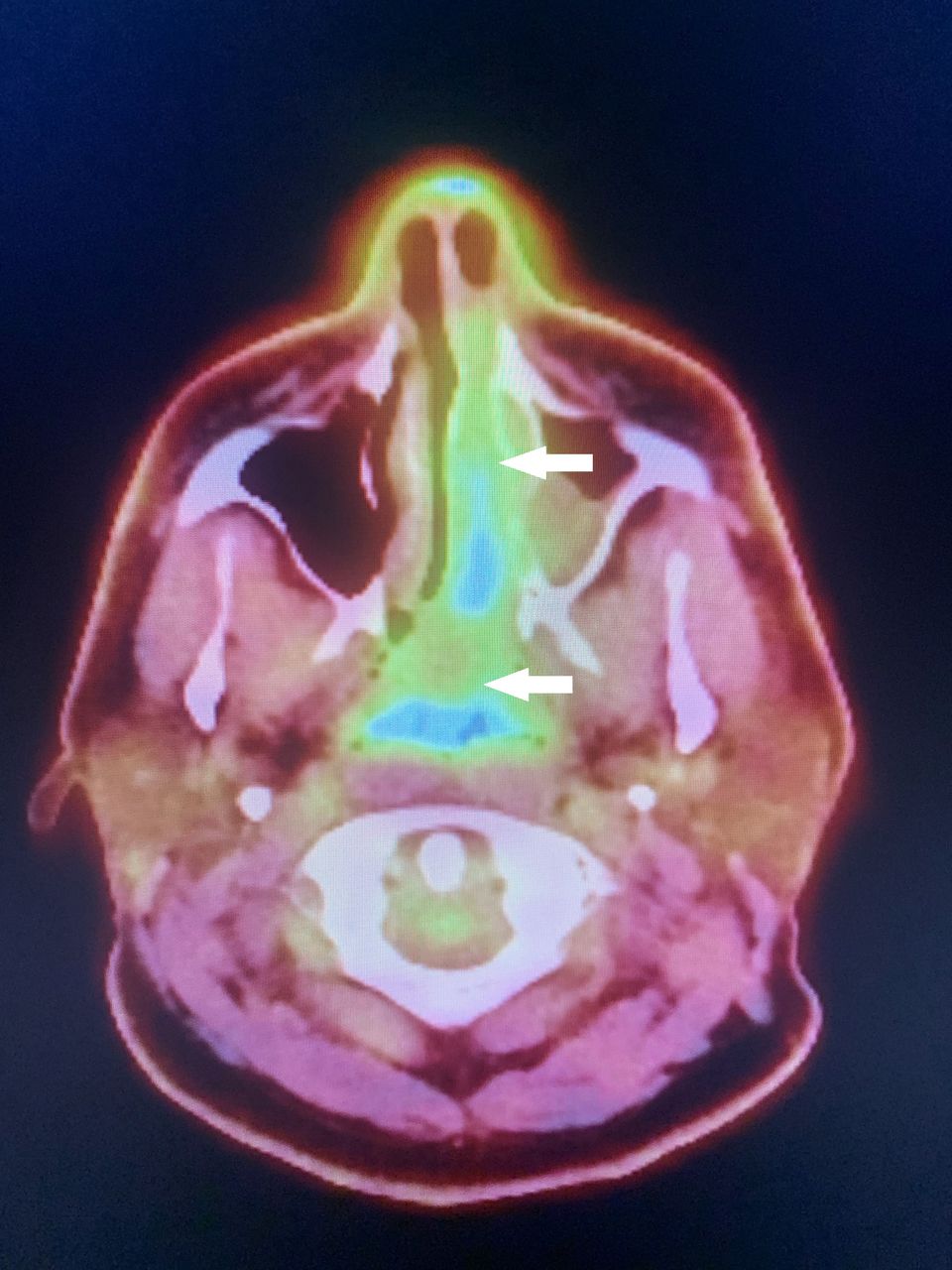
Once the imaging of the primary site was obtained, we completed the staging with a PET/CT scan, given the large size of the tumour and its very aggressive nature. The PET/CT revealed an irregular expansile hypermetabolic mass within the left nasal cavity and left maxillary sinus, causing osseous erosion of the left maxillary sinus medial wall. The mass extended slightly past the midline in the posterior nasopharynx, superiorly involving the left ethmoid sinus and inferiorly extending to the palate level (ie, the floor of the nose) (figure 2).

PET/CT image showing large irregular expansile hypermetabolic mass within the left nasal cavity and left maxillary sinus, causing osseous erosion of the left maxillary sinus medial wall (white arrows).
The PET/CT scan also showed a thyroid nodule and a very small sclerotic lesion without fluorodeoxyglucose activity affecting the second lumbar vertebrae. The patient’s thyroid had been biopsied in the past and he had been diagnosed with benign goitre. A biopsy of the L2 sclerotic lesion was performed and did not show evidence of malignancy.
He underwent resection of the tumour, including an ipsilateral medial maxillectomy, total ethmoidectomy, septectomy and anterior skull base resection. The procedure was complex, requiring the joint efforts of an otolaryngologist and a neurosurgeon via an endonasal approach.
Pathological description
The histopathologic pictureshowed a variable epithelial, neuroendocrine–neuroectodermal and mesenchymal differentiation pattern. The epithelial component included both squamoid (mostly fetal type or immature) cells with clear cytoplasm. These areas were positive by immunohistochemistry for AE1/3, CK7, MNF116, P63 and CDX2. The neuroendocrine–neuroectodermal component was synaptophysin, chromogranin, AE1/3, MNF116, CD56, calretinin and S100 positive, and the nuclei had the typical salt-and-pepper type of chromatin pattern. The mesenchymal component consisted of hypercellular areas of spindle cells with increased mitoses without a specific type of differentiation (such as skeletal muscle, cartilage, fat, etc). These areas were positive for androgen receptor and desmin, and SOX10 and myogenin were negative. Overall, the findings were consistent with the diagnosis of SNTCS, also referred to as malignant teratoma. (In earlier reports, other names such as teratocarcinoma, blastoma, carcinosarcoma, teratoid carcinosarcoma mixed mesodermal tumour and malignant mixed tumour were used; however, the more modern term teratocarcinosarcoma has replaced them4).
Pathological examination
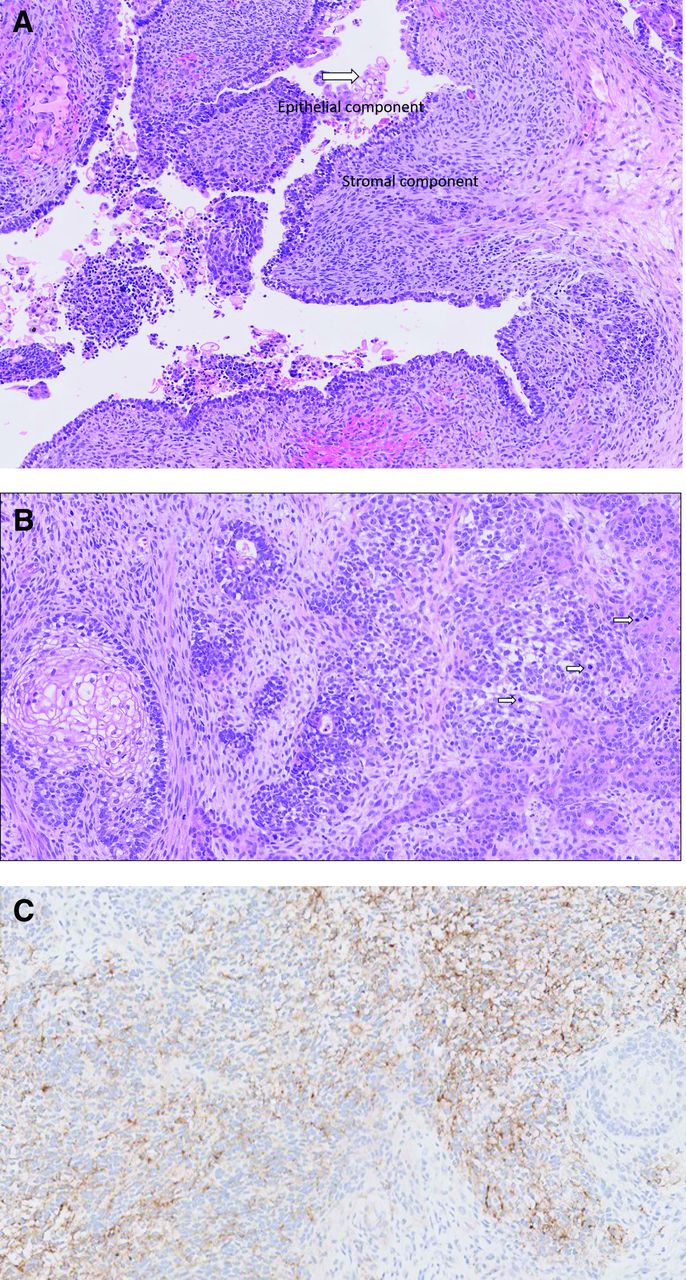
The patient recovered well from the procedure, without any complications. The final pathology reported teratocarcinosarcoma (figure 3A–C).

{kind=link}
{kind=link}
{kind=link}
(A) H&E. Epithelial and stromal components. Arrow indicates clear fetal- like cells. (B) H&E. Arrows indicate numerous mitoses. (C) Synaptophysin within the epithelial component.
Molecular analysis of the tumour revealed the following:
DNMT3 deletion exon 4–15.
KDM6A G5fs*15.
SMARCA4.
Differential diagnosis
Differential diagnoses of SNTCS include malignant craniopharyngioma, small cell carcinoma, poorly differentiated squamous cell carcinoma, sinonasal undifferentiated carcinoma, olfactory neuroblastoma, immature teratomas and carcinosarcoma. Given the rarity of the disease, they are usually misdiagnosed. Consequently, an adequate tissue sample and an expert review by a well-experienced pathology team are essential.3
Treatment
His case was discussed at the multidisciplinary sarcoma tumour board that recommended concurrent chemotherapy and radiation as adjuvant options following the treatment outlined by previous case reports.
The patient agreed with the treatment, and he received 60 Gy in 30 fractions, directed to the tumour bed and 54 Gy to the bilateral neck with concurrent weekly carboplatin AUC 1 plus paclitaxel 30 mg/m2.
Based on the pattern of nodal involvement of nasopharyngeal cancer and the anatomical lymphatic drainage,5 the team and the patient agreed on prophylactic neck lymph node irradiation at a low dose. The high-risk radiation volume was defined as the postoperative tumour bed, nasopharyngeal space (due to posterior nasopharyngeal involvement), nasal cavity and the involved paranasal sinuses. The low-risk volume is defined as areas at risk near critical structures such as the brainstem, optic nerves and optic chiasm.
Chemotherapy (weekly):
Carboplatin AUC 1 (150 mg).
Paclitaxel 30 mg/m2 (66 mg).
The patient received weekly chemotherapy for 6 weeks.
The patient had an excellent tolerance to treatment, only experiencing grade 1 mucositis, well managed with topical analgesics and supportive care.
Outcome and follow-up
Fifty months after the treatment, the patient is doing very well, with no sequelae and no evidence of recurrence/metastasis. He can perform all daily living activities without restriction. His sense of smell was partially affected.
Discussion
Heffner et al coined the term ‘teratocarcinosarcoma’ to describe these tumours based on the clinicopathological findings of a study of 20 cases.4 Clinically, the most common presenting symptoms are nasal obstruction (61.9%) and recurrent epistaxis (53.5%), according to the cases reported so far due to the tumour’s aggressiveness and rapid growth.6 When the tumour invades surrounding tissues, symptoms such as dysphagia, odynophagia, headaches, epiphora, vision loss, exophthalmos, anosmia, facial swelling, proptosis or even altered mental status are possible. Fluctuating hyponatremia due to the syndrome of inappropriate antidiuretic hormone secretion has also been reported in one case.6
Rao et al published on the largest cohort to date. It included 107 SNTCS cases (from 1968 to 2020). They found that the primary treatments used in those patients were surgical resection (87.2%), radiation therapy (59.3%) and chemotherapy (18.6%).7 The main treatment option is surgery, with negative margins. However, due to the anatomical complexity of the nasal sinuses, surgery does not always achieve complete tumour resection with negative margins; as such, neoadjuvant chemoradiotherapy plus surgical resection is the recommended therapy, with a nearly 88% survival rate after an average of 32 months, as compared with patients treated with surgery and radiation only, who had a 56.5% survival rate at 45 months.8
As the adjuvant radiation with or without chemotherapy showed a survival and possible local control advantage compared with surgery alone,9 the suggested target volume delineation is unclear. Most of the previously published case reports and case series did not clearly define the target volumes.
Due to the aggressiveness of SNTCS, cellular heterogeneity, involvement of the nasopharynx and anatomical lymphatic drainage,10 comprehensive radiotherapy to cover the base of the skull, nasopharyngeal space, parapharyngeal space, nasal cavity, the involved sinuses and the neck lymph nodes from Ib to V is recommended according to the base of skull/head and neck radiation principles.
We will emphasise the importance of discussing these cases at a specialised multidisciplinary tumour board, as there is evidence of improved patient outcomes.11 Further studies are needed to clarify the optimal use of radiation therapy and chemotherapy.
Learning points
Sinonasal teratocarcinosarcomas (SNTCSs) are rare high-grade tumours with histological features of carcinomas, sarcomas and teratomas.
The optimal treatment for SNTCSs is yet to be defined; however, a multidisciplinary approach is recommended.
SNTCS patients should receive treatment at an institution with access to an experienced team including surgeons, radiation oncologists and medical oncologists.
Further research is needed to optimise outcomes for SNTCS patients.
Ethics statements
Patient consent for publication
Footnotes
Twitter @gtinocomd
Contributors GPS, KD, RLC, LS, DMB and GT contributed to the discussion, material preparation, literature review and writing of this paper. All authors read, revised and approved the final manuscript and figures.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.