Article Text

Statistics from Altmetric.com
Description
A man in his 50s was referred for management of cutaneous sarcoidosis diagnosed on skin biopsy. He had developed numerous asymptomatic red skin lesions over the previous 2 months. Widespread red nodules involved nearly the entire skin surface (figure 1), including sparse lesions on the palms (figure 1C). The soles of the feet were not affected. Inguinal lymphadenopathy was noted.

Clinical and dermoscopical images of skin lesions. (A) Generalised nodules, (B) close-up of nodules, (C) sparse lesions on the palms and (D) dermoscopy showing arborising sharply demarcated vessels on a salmon-coloured background.
Dermoscopical examination of the skin lesions was performed as the rash was not typical for sarcoidosis, in which yellow-brown, ‘apple jelly’ nodules are characteristic. Salmon-coloured nodules with arborising, sharply demarcated superficial vessels (figure 1D) were seen. On specific questioning, there was a history of an initial penile lesion 2 months prior to the onset of the rash, which led us to the possibility of syphilis.
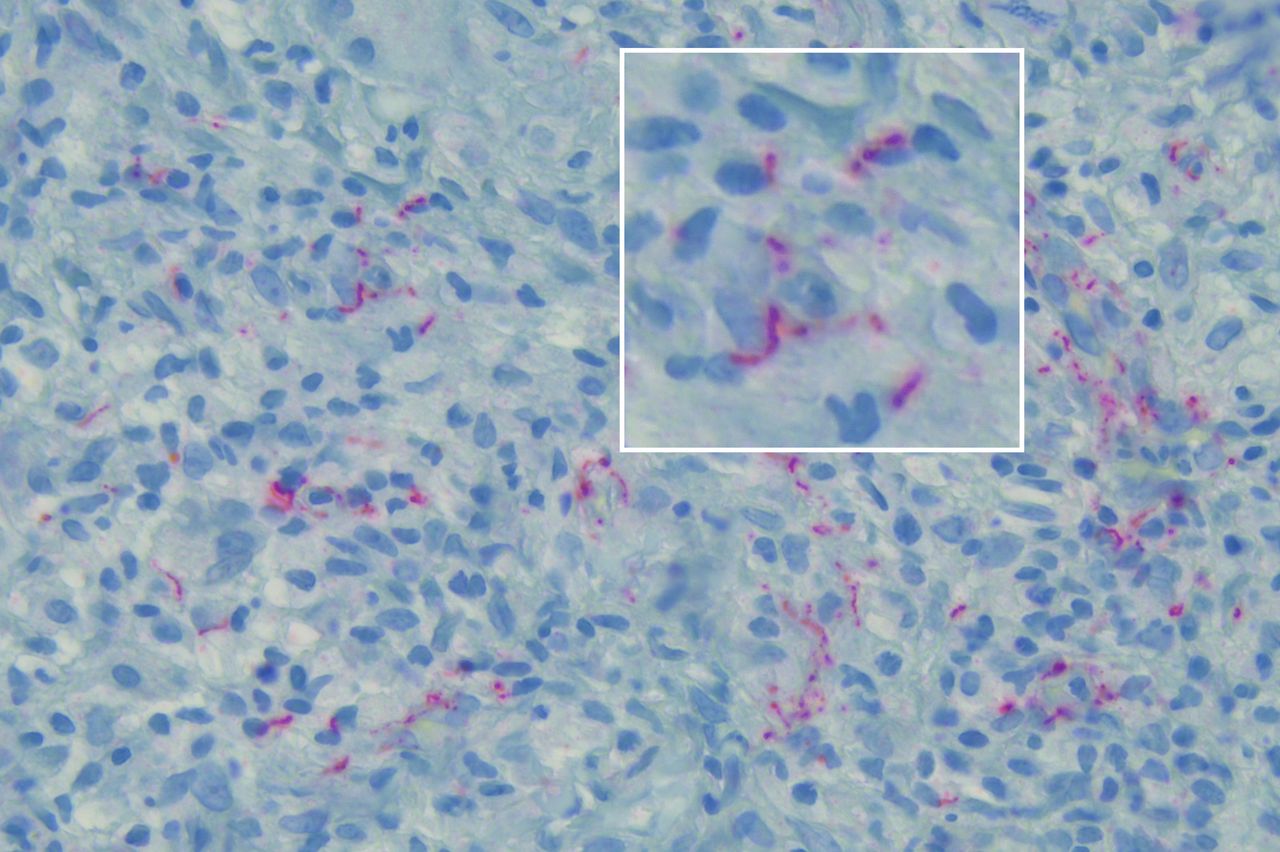
Immunohistochemistry of a new skin biopsy demonstrated spirochaetes consistent with Treponema pallidum within multifocal histiocytic dermal granulomas (figure 2). Syphilis was confirmed on serology with positive T. pallidum particle agglutination test (TPPA, 1:163 840) and venereal disease research laboratory (VDRL, 1:512). Further investigations for sarcoidosis, HIV, aortic aneurysm and eye involvement were negative.
{kind=link}
{kind=link}
Immunohistochemistry of skin biopsy demonstrating spirochaetes.
A diagnosis of nodular secondary syphilis was made and contact tracing initiated. Benzathine penicillin 2.4 million units intramuscular was administered at weekly intervals for 3 weeks due to the severity of the rash. A Jarisch-Herxheimer reaction was prevented by coadministration of oral glucocorticoids. There was a slow steady improvement in the skin lesions. Four weeks after initiating treatment, there was a three-step reduction in VDRL titre (1:512 to 1:64).
Secondary syphilis presents weeks to months after initial infection and is highly infectious. The typical rash of secondary syphilis is a diffuse exanthem of red-brown scaly macules and/or papules on the trunk and extremities. Nodular secondary syphilis is uncommon.1–3 Pruritus may result in excoriation, ulceration or crusting of the papules and nodules. The distribution may spare the palms and soles, or show only sparse lesions as in our patient.4 The colour of the nodules can vary from skin-coloured to violaceous or erythematous.
Histology of secondary syphilis also shows considerable variability. Although the typical pattern is a superficial and deep perivascular dermatitis with lichenoid vacuolar interface changes, in late secondary and tertiary syphilis granulomas of epithelioid and multinucleated histiocytes can be found. Interspersed plasma cells are typical of secondary syphilis compared with sarcoidal granulomas which are often naked with only a few lymphocytes and multinucleated giant cells. Necrosis is not seen in the granulomas of secondary syphilis or sarcoidosis but are typical in tertiary syphilis. Dermoscopy is useful in evaluating skin nodules such as sarcoidosis and cutaneous B cell lymphoma. Dermoscopical features of nodular secondary syphilis have not been previously described. Arborising sharply demarcated vessels on a salmon-coloured background are a possible key feature of the diagnosis.
HIV status should be checked in all patients with syphilis, and coexistence of nodular syphilis with HIV has been described on several occasions. Benzathine penicillin remains the treatment of choice for nodular secondary syphilis. Our case again demonstrates syphilis is the great imitator, on this occasion presenting with skin nodules diagnosed as cutaneous sarcoidosis. Treating physicians should be aware of unusual clinical manifestations of syphilis and consider this during their everyday routine. Dermoscopy can be a useful tool for the diagnosis of nodular secondary syphilis.
Patient’s perspective
Initially I felt uncomfortable with the diagnosis of syphilis, which was accompanied by a difficult consultation regarding sexual contacts. With time, a trusting relationship was established with the medical staff and I came to understand the disease, which is crucial in the management of sexually transmitted diseases.
Learning points
Syphilis is the great imitator and can present with cutaneous nodules resembling sarcoidosis.
History of a genital lesion and the widespread distribution of skin lesions should prompt investigation for syphilis, including serology and treponema stain on skin biopsy.
Arborising sharply demarcated vessels on a salmon-coloured background on dermoscopy are a possible key feature for the diagnosis of nodular secondary syphilis.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Delwyn Dyall-Smith for her great support in writing this paper.
Footnotes
Contributors FVK: conceptualisation, data curation, investigation, project administration, visualisation, writing. RC: data curation, investigation, project administration, supervision. BC-S: data curation, investigation, visualisation. WS: conceptualisation, data curation, investigation, project administration, supervision, visualisation, writing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.