Article Text

Statistics from Altmetric.com
Description
A man in his early 60s presented to the hospital with complaints of pain in right hypochondrium in the subcostal region for 2 months. No other significant history was present. On local examination, mild local tenderness was present along the right lower ribs. His routine blood investigations were within the normal limit.
Ultrasound revealed cortical irregularity with ill-defined hypoechoic soft-tissue along the right 10th rib.
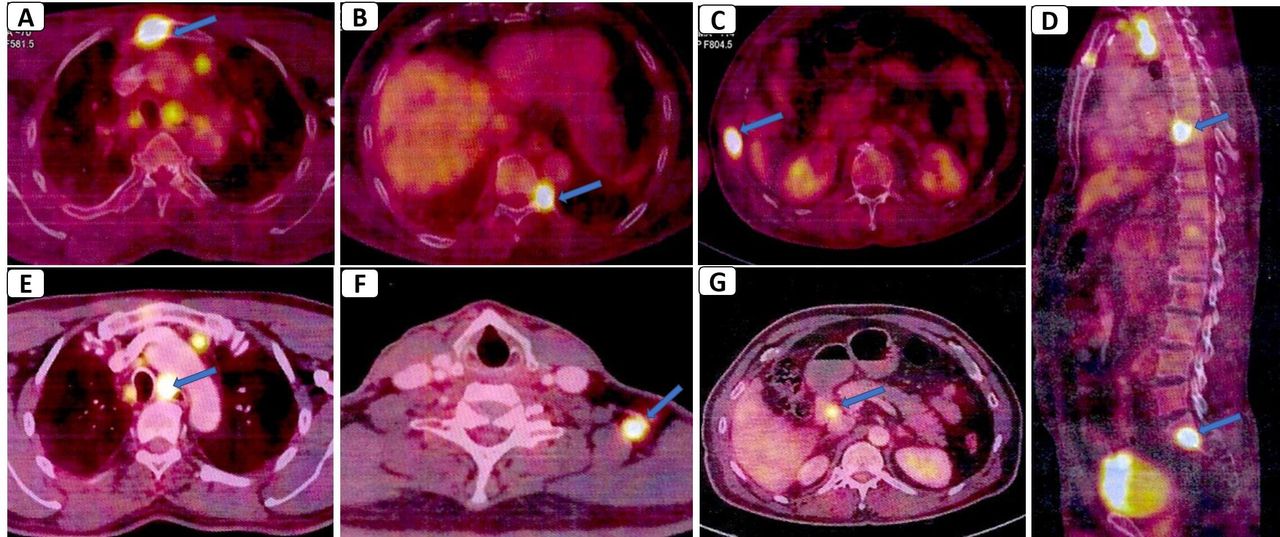
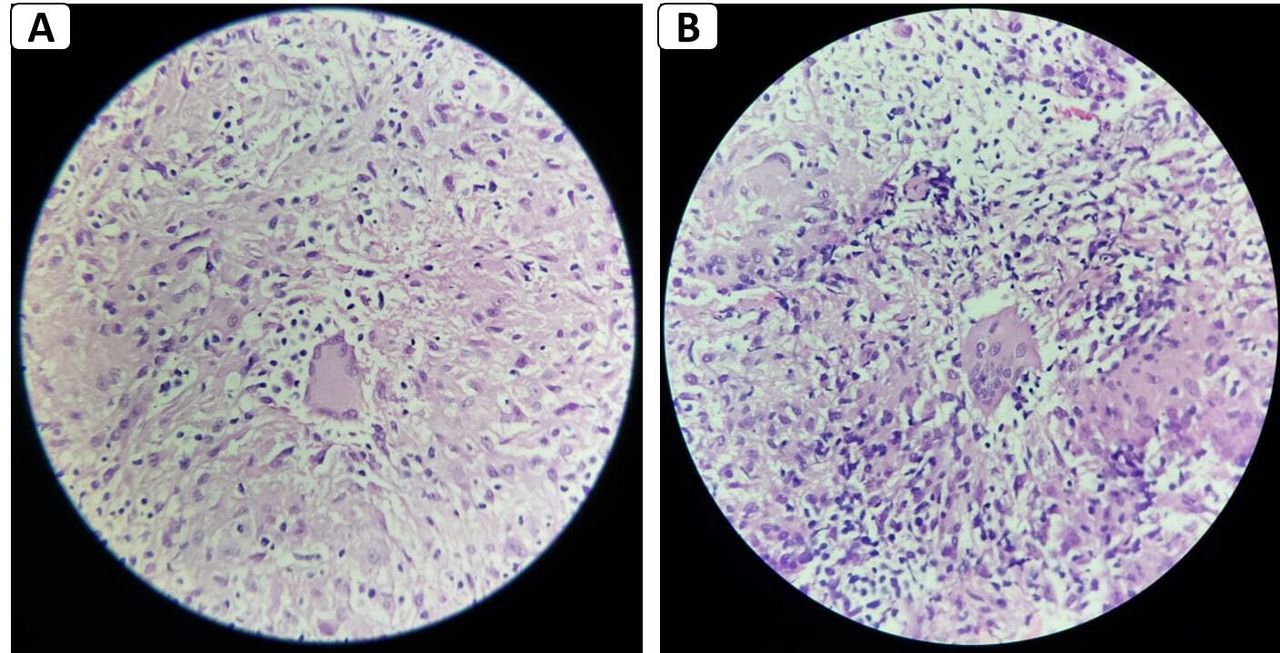
For further evaluation, contrast-enhanced CT (CECT) thorax and abdomen were done. CECT (figure 1) revealed multifocal lytic and expansile lesions with minimal enhancing soft-tissue components in right 10th rib, left 5th rib, 8th vertebral body, left 9th costovertebral junction and in the sternum towards the 2nd right costotransverse junction. Few enlarged non-necrotic discrete paratracheal left supraclavicular and periportal lymph nodes were seen at the largest 11 mm in the short axis dimension. Both lungs and all abdominal organs were normal. Based on CECT findings, the possibility of metastasis and multiple myeloma was kept and further evaluation with positron emission CT (PET-CT) was ordered. PET-CT (figure 2) revealed metabolic activity in all the above-described lesions seen on CT. Additional fluorodeoxyglucose (FDG) avid lytic lesions were present on PET-CT in the sacrum, lumbar vertebra and bilateral iliac blades, which were not visualised on CECT. However, a primary tumour was not detected. CT guides biopsy was done on the lytic lesion in the sternum and from the left supraclavicular lymph node. Histopathological examination (figure 3) revealed the presence of granulomatous inflammation with Epithelioid granuloma, multinucleated giant cells and lymphocytes. Although Zeihl Neelsen staining was negative, the PCR test for mycobacterium tuberculosis (TB) was positive. Anti-TB combination therapy was started and after 2 months of treatment, rib pain gradually subsided.
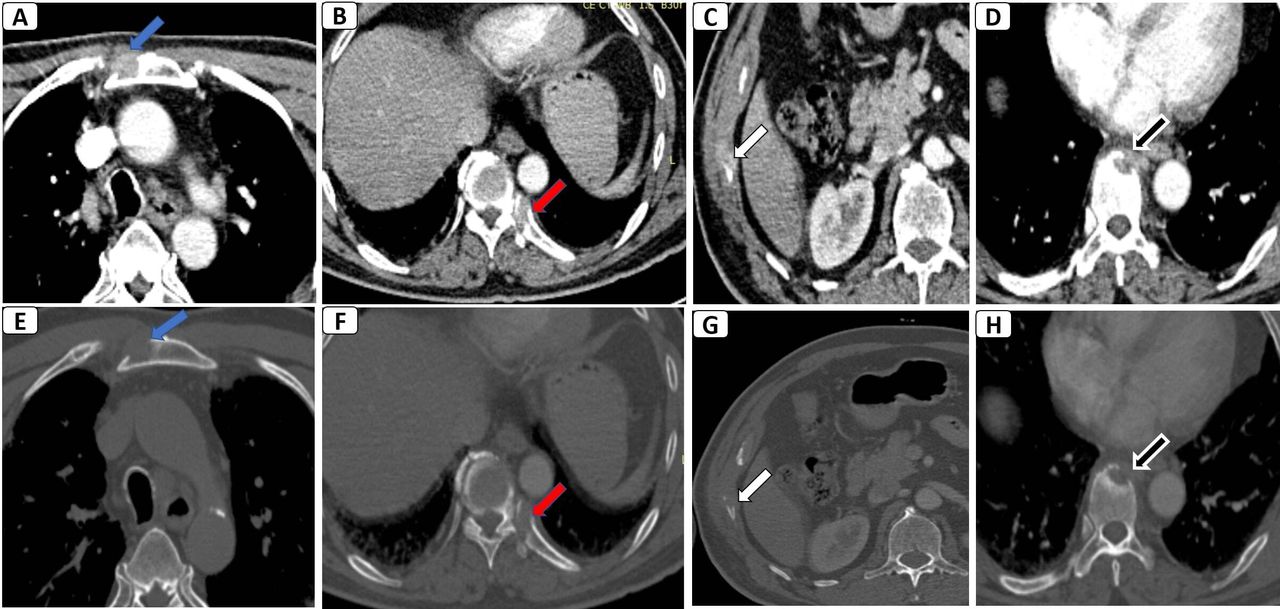
Contrast-Enhanced CT of chest and abdomen. Soft-tissue window (A–D), and corresponding bone window (E–H) images demonstrate multifocal lytic and expansile lesions with minimal enhancing soft tissue component in the sternum (blue arrows), left 9th costovertebral junction (red arrows), right 10th rib (white arrows) and eighth vertebral body (black arrows).

Whole-body positron emission CT (A–G) shows multifocal fluorodeoxyglucose (FDG) uptake (blue arrows) in the sternum, left ninth costovertebral junction, right 10th rib, eighth vertebral body, sacrum. FDG uptake was also seen in a few mediastinal lymph nodes (E), left supraclavicular (F) and periportal lymph nodes (G).

{kind=link}
{kind=link}
{kind=link}
Histopathological images (A, B) show central necrosis, Langhans-type giant cells, epithelioid cells and multiple lymphocytes suggesting granulomatous inflammation. (H&E, ×80).
Extrapulmonary primary skeletal TB is a rare form of TB representing 1%–2% of all TB cases.1 Tubercular spondylitis is the most common form of skeleton TB, which on imaging shows subligamentous spread with contiguous vertebrae involvement, endplate irregularity and paraspinal abscess. However, non-contiguous and multifocal involvement seen in this case is very unusual for TB, especially in an immunocompetent patient. The CT imaging appearance of this case is more typical for metastatic disease and multiple myeloma leading to its misdiagnosis. Although a high standardised uptake value (SUV), greater than 2.5, is described in malignant lesions, there are multiple reports of much higher values in TB.2 Thus, differentiation of metastatic and infective lesions based on FDG uptake and SUV is not possible on PET-CT. Histopathological and microbiological examinations are always required to make a correct diagnosis. There are very few previous case reports of multifocal osteolytic tubercular bony lesions in the literature.3–5 Knowledge of the imaging appearance of this rare form of skeleton TB is important, and TB should also be kept as differentials on imaging in addition to malignant disease in such a scenario.
Patient’s perspective
I developed pain in my right lower chest for about a month. After local examination, I underwent an ultrasound in which there was suspicion of some bony lesion. Further CT and PET-CT were ordered which further raised the suspicion of the neoplastic lesion. My family and I were very tense about this news. We were referred to a cancer hospital for further investigation. Here they did a biopsy on my chest. Biopsy reports revealed it to be a tubercular lesion. I am on anti-tubercular treatment and after two months of treatment, I am completely fine. I am very thankful to all the doctors and their teams who diagnosed my condition and excluded the possibility of neoplastic disease.
Learning points
Multifocal osteolytic non-contiguous tubercular bony lesions are a rare form of skeleton tuberculosis, which closely mimics metastasis on imaging.
Radiological imaging and positron emission CT are misleading in such cases; therefore, histopathology and microbiological investigation are required for making the diagnosis.
Ethics statements
Patient consent for publication
Footnotes
Contributors Data were compiled and report was written by PS. MK helped in inception of report, image collection and final review. The manuscript revision and the final correction were done by PK and SPS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.