Article Text

Abstract
The case of a female patient in her 50s presenting as a surgical emergency with abdominal pain and a positive Obraztsova’s sign. Seven days prior to the presentation, a lumbar puncture (LP) had been performed to investigate severe headaches and exclude a subarachnoid haemorrhage. The patient was subsequently found to have an acute lumbar arterial bleed causing haemodynamic instability and a psoas haematoma. An emergency lumbar artery embolisation procedure was performed by the interventional radiology department in order to stabilise the bleed. The patient made a full recovery prior to discharge.
- general surgery
- interventional radiology
- neurology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Despite the rarity of psoas haematomas, with an incidence of 0.1%–0.6%,1 the condition potentially carries a significant mortality and morbidity, with studies showing mortality rates varying widely between 3% and 30% and worse prognosis generally reported in intensive therapy unit cohorts.2 The causes can be divided into traumatic and non-traumatic aetiologies. This case describes a traumatic iatrogenic psoas muscle haematoma as a complication of a lumbar puncture (LP) procedure. There were no similar cases found in the literature search performed. A detailed clinical history, thorough examination and a review of recent interventions are all vital for early diagnosis and treatment of this disorder.
Case presentation
A female patient in her 50s was referred to the general surgical on call team presenting with a gradually worsening 7-day history of right-sided abdominal and lumbar pain which radiated down her right thigh, with positive Obraztsova’s sign. Her medical history included multiple presentations with adhesional small bowel obstruction secondary to previous endometrial ablation surgery with post op complications. A week prior to presentation, she had attended hergeneral practitioner (GP) complaining of sudden onset severe occipital headache associated with photophobia, vertigo and paraesthesia. Due to a family history of cerebral aneurysms, her GP urgently transferred her to an emergency department, where she was subsequently admitted under the acute medical team. There was no evidence of haemorrhage, space-occupying lesion or acute events on the CT head scan; as such, a lumbar puncture was ordered to rule out a subarachnoid haemorrhage (SAH). The lumbar puncture proved to be technically challenging, requiring three attempts to obtain a sample. However, the cerebral spinal fluid (CSF) sample obtained could not be analysed due to the high quantity of blood, which was suggestive of a traumatic tap. Therefore, a CT angiogram of the head was performed, revealing a 1–2 mm aneurysm projecting from the communicating segment of the right internal carotid artery. The findings were discussed with the neurosurgical department, and a repeat LP was advised. This was duly performed and showed no evidence of a SAH. As a result, the patient was discharged with a plan for a repeat CT angiogram in 12 months, as well as neurosurgical follow-up.
Seven days later she presented with right-sided abdominal and back pain radiating down her right leg and was admitted to the surgical ward. On examination she was tender in the right flank and right iliac fossa.
Investigations
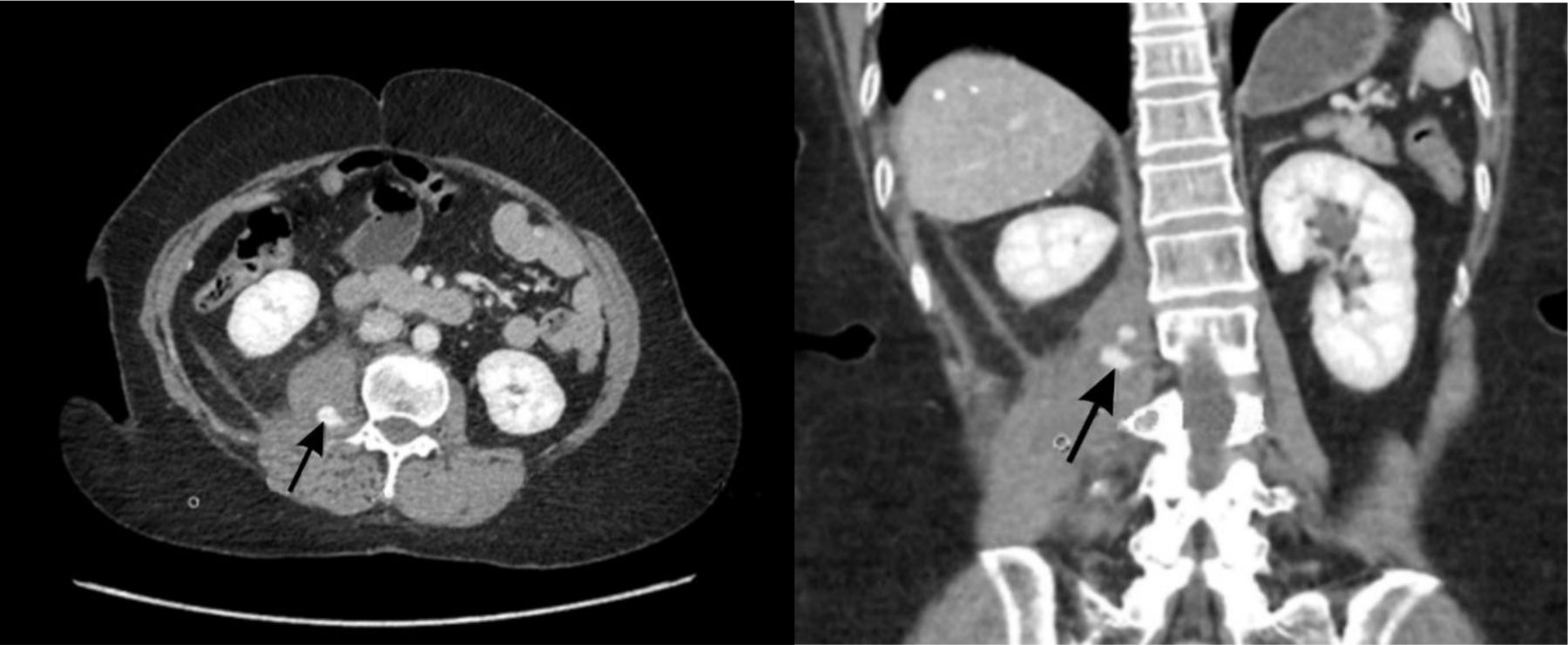
The patient was investigated with a CT abdomen and pelvis with contrast. This revealed a right psoas haematoma associated with active haemorrhagic focus in its superior aspect, as well as a partial small bowel obstruction. Routine blood tests also showed a drop in haemoglobin from 123 g/L to 93 g/L. This supported the diagnosis of an active bleed, as suggested by the CT scan. The images below are snapshots taken from the patient’s CT scan which show contrast extravasation into the right psoas muscle (figure 1).

CT scan of the abdomen and pelvis showing contrast extravasation into the right psoas muscle on axial and coronal views (indicated by black arrow).
Differential diagnosis
Due to the patient’s presentation and medical history, the differential diagnoses considered include an abdominal aortic aneurysm, pyelonephritis, acute appendicitis, and adhesional small bowel obstruction. CT scan of the abdomen and pelvis confirmed the diagnosis of the latter, in addition to a right psoas haematoma associated with an active haemorrhagic focus.
Treatment
The patient was discussed with the interventional radiology department, with embolisation of the lumbar artery deemed the treatment of choice. During the procedure, angiography revealed a pseudoaneurysm arising from the right L2 lumbar artery, which was successfully embolised. Following the procedure, there was no flow into the artery and the aneurysm showed stasis of the contained contrast.
Outcome and follow-up
After the embolisation was performed, the patient’s observations and repeat haemoglobin results showed haemodynamic stability. This indicated that the active bleeding into the psoas haematoma had resolved. However, the concurrent partial small bowel obstruction took 8 days to fully resolve, during which the patient remained in hospital.
Discussion
A lumbar puncture procedure is an important diagnostic tool for detecting central nervous system (CNS) infections (bacterial, viral and fungal), CNS malignancies, subarachnoid haemorrhages and certain demyelinating condition.3 The procedure is also used therapeutically for patients requiring spinal anaesthesia and intrathecal administration of medications.4 One of the complications for which patients are consented prior to the procedure is bleeding; rare complications associated with this are usually secondary to spinal haematomas. Indeed, even spinal haematomas were found in one series only to have occurred in 2% of patients undergoing a LP while taking anticoagulant therapy.5 No similar cases of psoas haematomas post LP were found in the literature search. However, cases of retroperitoneal haematomas resulting from LPs can be found in the literature available, with the first case described in 1950.6 As such, it is difficult to determine the incidence of this complication; case reports of retroperitoneal haemorrhage were found only sporadically in the literature search.
Psoas haematomas are a rare occurrence, with aetiology typically divided into traumatic and non-traumatic causes. These include trauma, iatrogenically from lumbar surgeries, use of anticoagulants and haematological disorders, such as disseminated intravascular coagulation and haemophilias.7 8
A LP procedure is an invasive test used to gain access to the subarachnoid space—in this case, in order to sample the CSF. Knowledge of the anatomy of the area and the performance of the procedure are crucial to understand how bleeding may have occurred in this case.
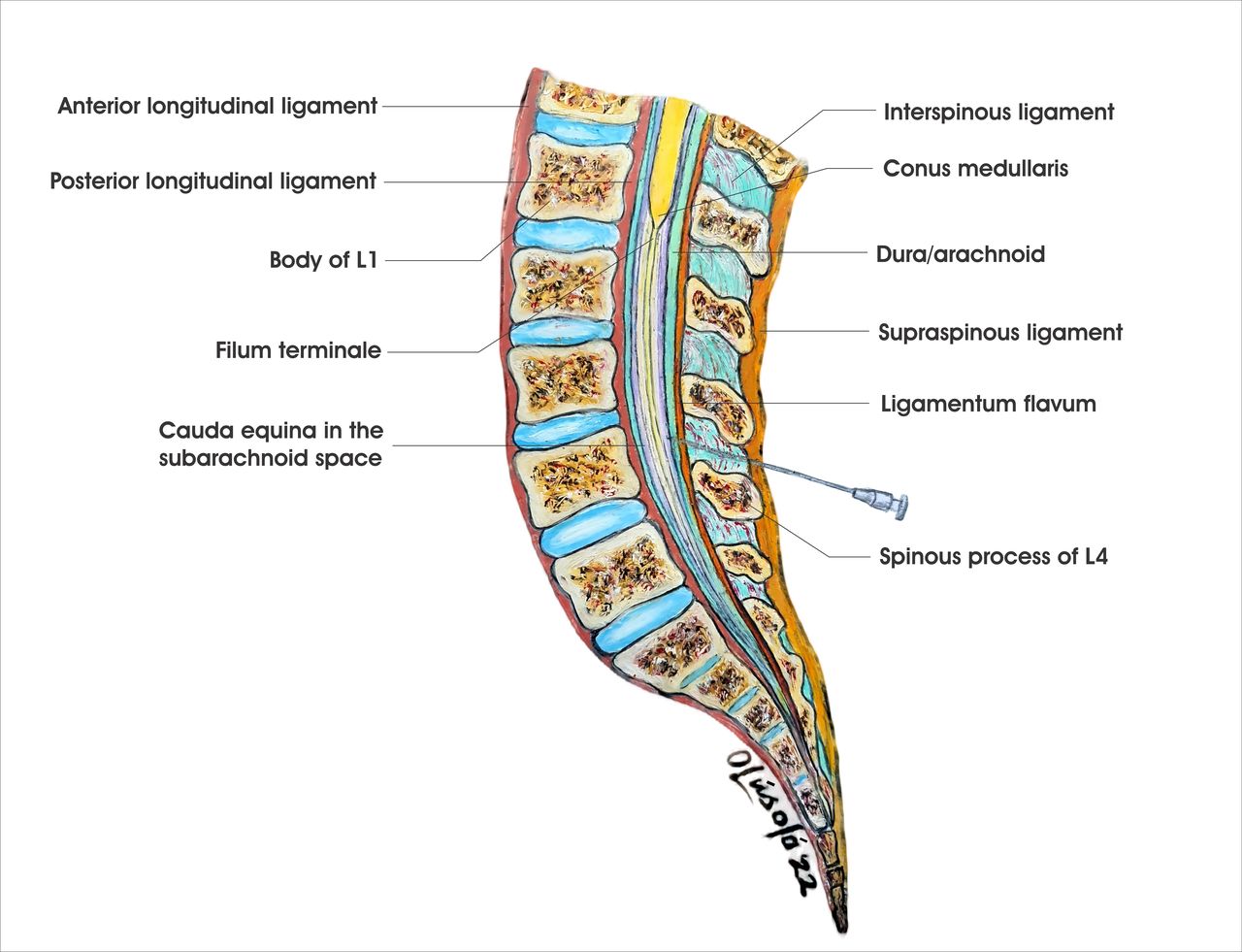
The first step in performing the procedure is marking the correct anatomical position of the insertion site. The insertion site is typically L3/L4 or L4/L5, as these points are below the termination of the spinal cord (see figure 2). The fourth lumbar vertebra is typically found by palpating the patient’s superior aspects of their iliac crests and drawing a line between these. It should be noted, however, that this line can intersect between L1 and L5; for example, the line has been found to join more superiorly than L4 in female patients and obese patients.9 10 Once the point of insertion has been found, a LP is typically performed with the patient’s neck, back and limbs in flexion so that they are in the foetal position. A spinal needle is then inserted until the subarachnoid space is reached and CSF begins to flow through the needle.

Mid-sagittal section through the lumbar spinal column.
As can be seen in figure 3, a transverse view of the point of insertion with surrounding structures and blood supply is useful to gain insight into what may have occurred in this instance; one possibility is an inadvertent violation of the paravertebral structures.
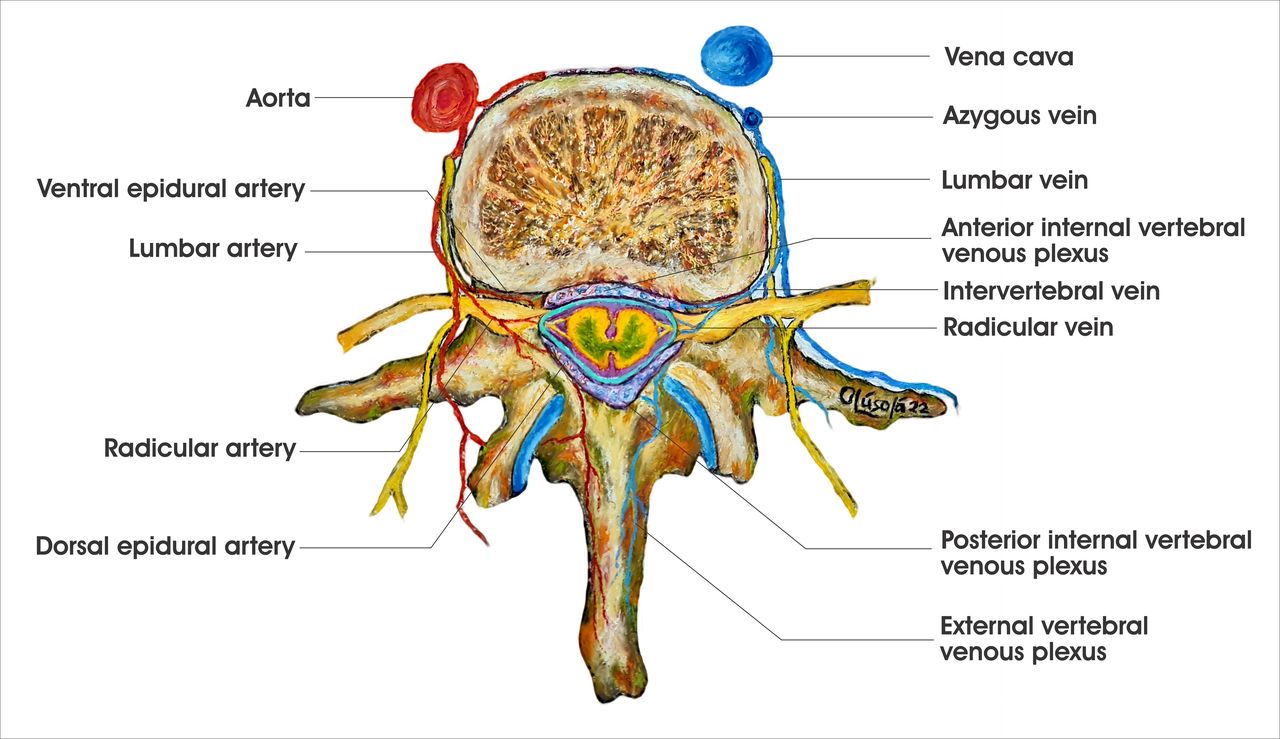
Transverse section demonstrating arterial and venous supply of the spinal cord.
The occurrence of a traumatic tap suggests that the needle may have been angled too far laterally into the area where the psoas muscle is attached along the lumbar vertebrae and the intervening discs. However, this may also indicate damage to the radicular or epidural vessels, or even the internal vertebral venous plexus if the needle was significantly advanced anteriorly.11 12 The psoas muscle occupies the gutter between the bodies and transverse processes of the lumbar vertebrae, with the lumbar plexus embedded within it and part of the external venous plexus lying posterior to it, just as the lumbar arteries with their accompanying veins.13 The close relation of the lumbar arteries with their posterior and spinal branches to the respective vertebrae (as they exit the abdominal aorta) leaves them at risk of injury during a LP.11 13 Figure 4, taken during the embolisation, shows extravasation of contrast from the lumbar artery at the level of L2, suggesting that it may have been damaged in this way.

Snapshot showing extravasation of contrast (black arrow) from the lumbar artery (white arrow) during embolisation.
The most common documented presenting symptoms of psoas haematomas are abdominal pain and features of hypovolaemia.7 8 14 Despite this, the patient presented in a less commonly reported manner with pain in the lower back and flank, which radiated down to the upper thigh and was associated with paraesthesia in the same area.7 8 13 This pain was aggravated by movement and bending forward but there was no neurological deficit. The neuropathic symptoms from psoas haematomas have been attributed to compression of the lumbosacral plexus by the haematoma, resulting in a rapid increase in pressure within the psoas muscle and the containing fascial compartment.15 Some patients diagnosed with psoas haematomas present with motor weakness of muscles supplied by the femoral and obturator nerves, but this is more often associated with large chronic haematomas.8
Furthermore, patients may have a variety of clinical signs, such as anaemia, demonstrable limb paresis, tendon reflex abnormalities, abdominal tenderness or flank ecchymosis. Nevertheless, diagnosis of a psoas haematoma is difficult using physical findings alone.13 This patient’s diagnosis was confirmed by a contrast-enhanced CT scan of the abdomen, although MRI has been argued to be more sensitive for such evaluation.8 The literature search revealed that most non-traumatic psoas haematomas resolve spontaneously without any adverse sequelae, while others can be managed with blood transfusion only.8 14 The patient had an active haemorrhagic focus on the abdominal CT scan, as well as a significant drop in the haemoglobin level; as such, further action by interventional radiology was crucial. Subsequently, a successful angioembolisation of the right second lumbar artery was performed, which fully resolved the symptoms (as seen in figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Snapshot showing embolisation of lumbar arterial bleed (as indicated by the black arrow).
Psoas haematomas may mimic other abdominal conditions. Given the non-specific nature of the clinical presentation, a high index of clinical suspicion is required to make the diagnosis.
Learning points
Psoas haematoma should be considered as a cause of back/abdominal pain following lumbar puncture even in patients who are not on anticoagulant or with a pre-existing coagulopathy.
Obtaining adequate history is key to arriving at a diagnosis, as exemplified by the old aphorism; listen to your patient, they are telling you the diagnosis.
As demonstrated in this case, an arterial injury may present in days and not necessarily a more acute presentation.
In the appropriate clinical context, a contrast-enhanced CT scan of the abdomen and pelvis should be obtained to exclude this treatable condition.
Measures to minimise the risk of complications and make lumbar puncture safer should be incorporated into guidelines, including methods to ensure the correct position of L3/L4 or L4/L5 is found, use of atraumatic spinal needles, and performing the procedure under ultrasound guidance.16 17
Ethics statements
Patient consent for publication
Acknowledgments
The authors acknowledge the valuable help of Dr Andrew Keane for reviewing the manuscript and making images available for the case report.
Footnotes
Contributors EO, ND and KamilaR: conceptualised the case report and drafted the manuscript. EO and KamilaR: literature review and radiology images. EO and KuranR: review of literature and drafting of discussion. EO, KuranR and KamilaR: review and editing. ND: review, editing and supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.