Article Text

Abstract
Chondromyxoid fibroma (CMF) is a rare, benign bone tumour most commonly located within the metaphyseal region of the long bones surrounding the knee joint. Here, we present an interesting case of a young woman in her early 20s with CMF of the left iliac bone and include a literature review of comparable studies with an emphasis on radiological findings and important differential diagnoses to be aware of in this atypical location.
- Orthopaedics
- Radiology
- Pathology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Chondromyxoid fibroma (CMF) is a rare, benign bone tumour, which constitutes <1% of all primary bone neoplasms. Peak incidence occurs in the second-to-third decade of life, with 75% of patients presenting before the age of 30 and men being more commonly affected than women (M:F=2:1). The typical presenting complaint is one of pain and/or swelling; however, smaller lesions can be asymptomatic. The lesion itself is most commonly located within the metaphyseal region of the long bones (60%), particularly surrounding the knee joint in either the distal femur or most classically within the proximal tibia (25%). Other locations may include the flat bones (40%) or small tubular bones of the hands/feet (17%); however, involvement of the pelvic bones specifically is extremely rare (10%).1
Ever since it was first described by Jaffe and Lichtenstein in 1948, clinical diagnosis has remained a significant challenge.2 First, its radiological findings are non-specific across all modalities. Second, the occurrence of CMF in older patients and/or in atypical locations such as the pelvis, where in both scenarios the incidence of malignant lesions such as chondrosarcoma (CS) is higher, and in the latter where benign lesions can grow to a larger size, can significantly alter the index of suspicion.3 Third, despite the fact that histological sampling is required for definitive diagnosis, cellular findings can still overlap, with the presence of large pleomorphic cells and/or cells with oval nuclei and longitudinal grooves simulating the appearances of CS and chondroblastoma (CB), respectively.4 5
Case presentation
A young woman in her early 20s with a history of rheumatoid arthritis presented to our rheumatology department complaining of worsening back pain and tenderness over the left sacroiliac joint. In light of the patient’s known inflammatory arthropathy the initial clinical suspicion was for an axial spondyloarthritis.
Investigations
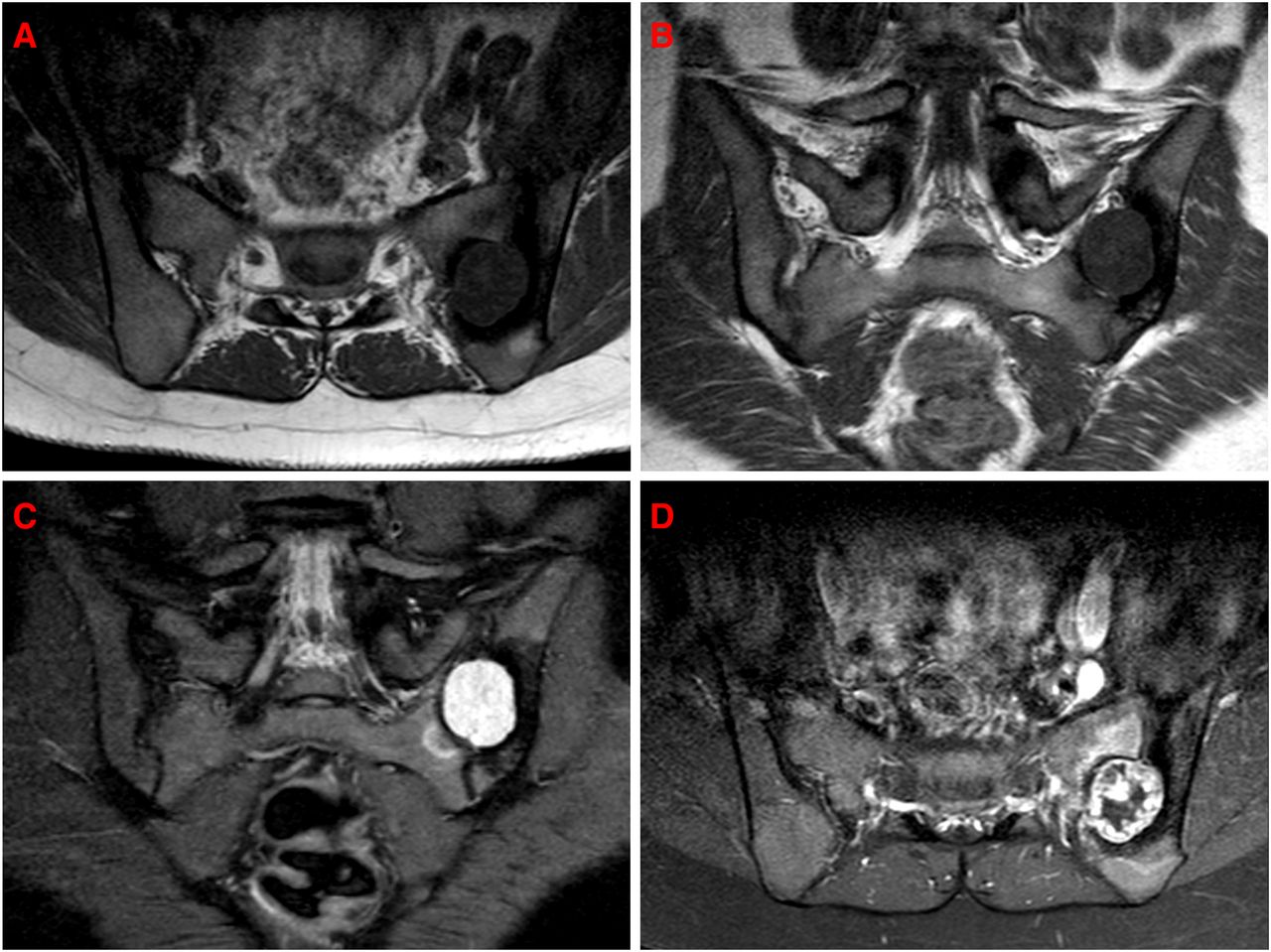
Initial blood tests were positive for antinuclear antibodies (ANA) but negative for anti-double stranded DNA (dsDNA) and anti-cyclic citrullinated protein (CCP) antibodies, rheumatoid factor (RF) and human leukocyte antigen (HLA)-B27. A precontrast and postcontrast MRI of the sacrum/pelvis was performed to assess for evidence of axial spondyloarthritis. The T1-weighted sequences showed a 27 mm × 24 mm × 29 mm (anteroposterior (AP) × transverse (TS) × craniocaudal (CC)), well-circumscribed, homogeneous, hypointense lesion centred over the posterior left sacroiliac joint with associated scalloping of the adjacent sacrum and ilium, and sclerosis of the ilium. The lesion demonstrated mildly heterogeneous but predominantly high signal on short tau inversion recovery (STIR)-weighted sequences and peripheral nodular enhancement following administration of intravenous contrast (figure 1).
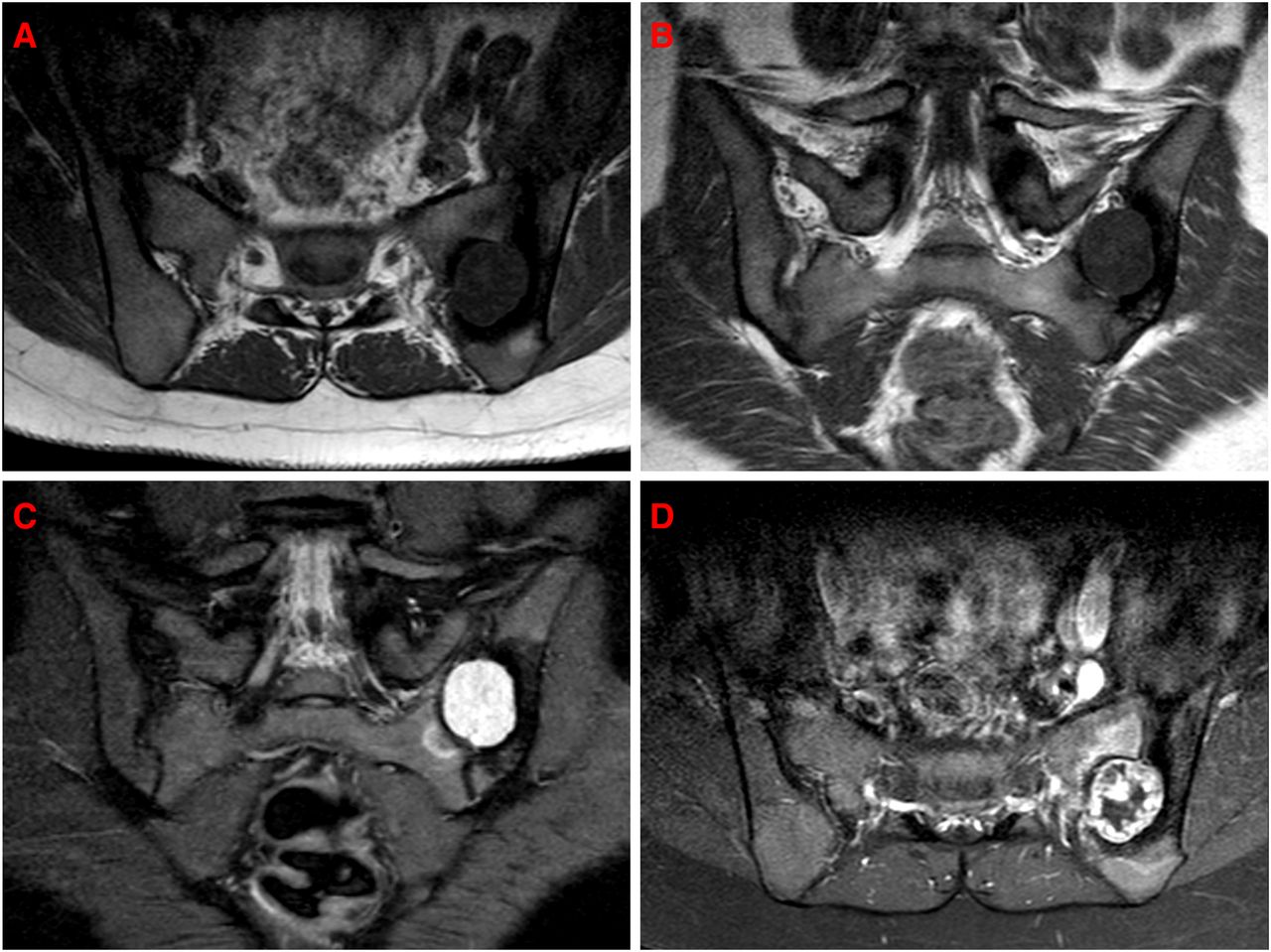
MRI of the sacrum/pelvis with (A) axial and (B) coronal precontrast T1 sequences, which show a 27 mm × 24 mm × 29 mm (AP × TS × CC), well-circumscribed, homogeneous, hypointense lesion centred over the left posterior sacroiliac joint with associated scalloping of the adjacent sacrum and ilium, and sclerosis of the ilium. (C) Coronal STIR sequence, which demonstrates a mildly heterogeneous but predominantly high signal throughout the lesion. (D) Axial postcontrast fat-saturated T1 sequence, which demonstrates peripheral nodular enhancement.
Of note, was a prior non-contrast MRI of the sacrum/pelvis, which had been performed 4 years earlier and showed a small area of non-specific bone marrow oedema at the same location (figure 2).

MRI of the sacrum/pelvis performed 4 years earlier with (A) coronal T1, (B) coronal STIR, (C) axial T2 and (D) axial T2 Dixon sequences, which show a small area of non-specific bone marrow oedema within the left ilium adjacent to the left posterior sacroiliac joint.
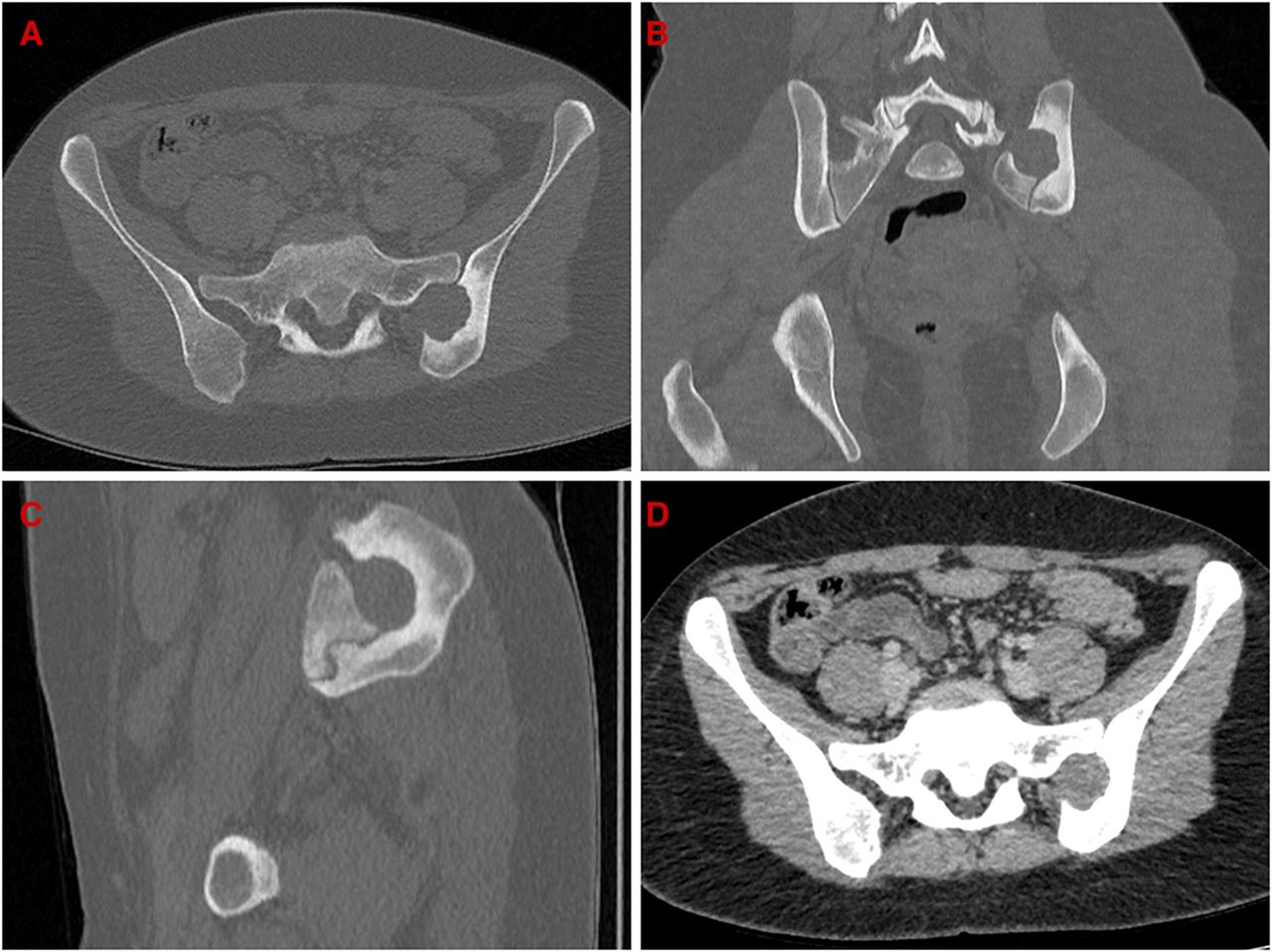
A CT scan was performed to evaluate the degree of bony erosion and to assess for intralesional calcification. This confirmed a soft tissue mass centred over the posterior left sacroiliac joint with marked bony erosion of the adjacent sacrum and ilium, and sclerosis of the ilium. No intralesional calcification, additional mass lesions or pelvic lymphadenopathy were demonstrated (figure 3).
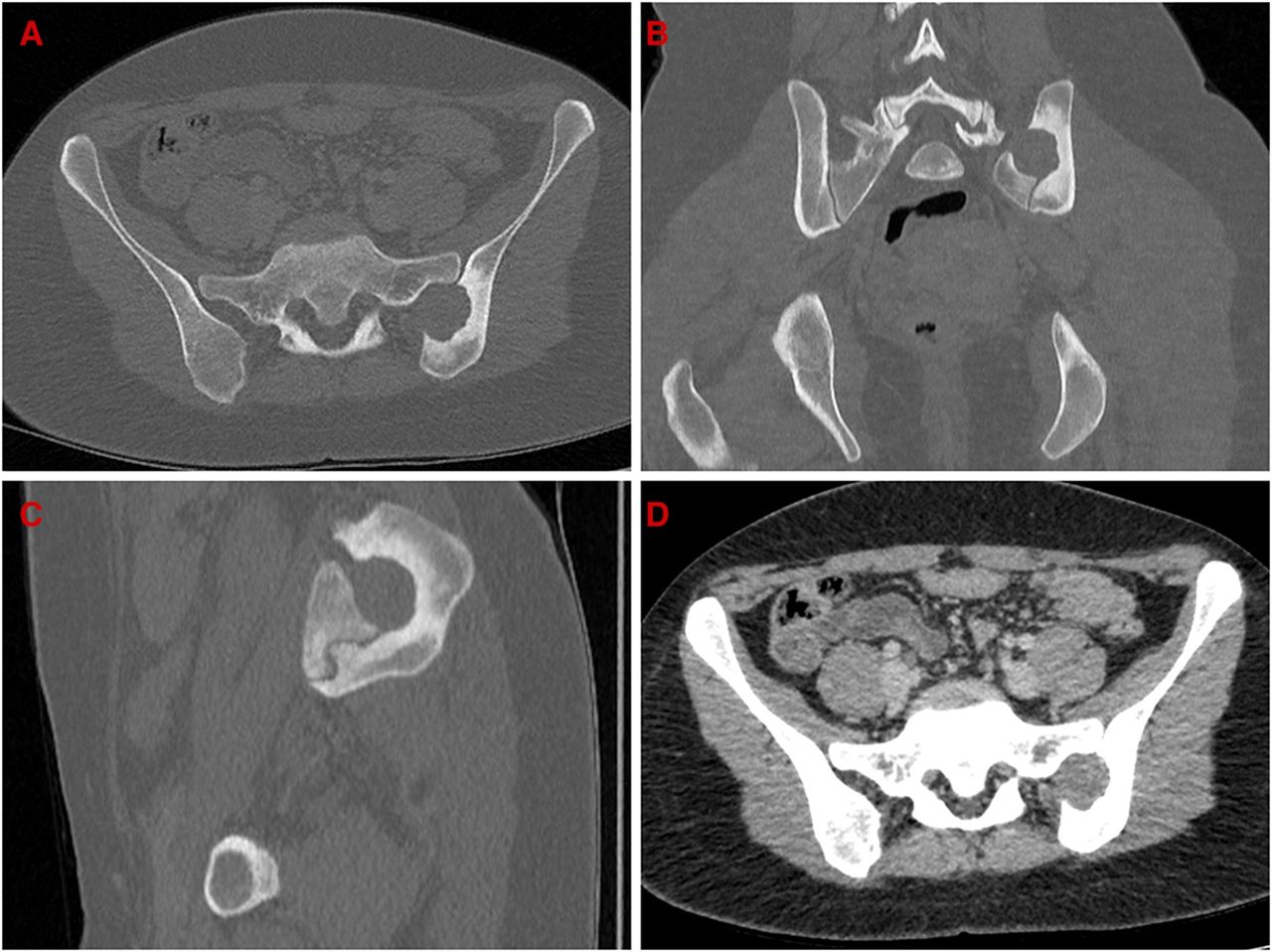
Non-contrast CT with (A) axial, (B) coronal and (C) sagittal bone windows, and (D) axial soft tissue windows, which confirm a lesion centred over the posterior left sacroiliac joint with marked erosion of the adjacent sacrum and ilium, and sclerosis of the ilium. No intralesional calcification, additional mass lesions or pelvic lymphadenopathy were demonstrated.
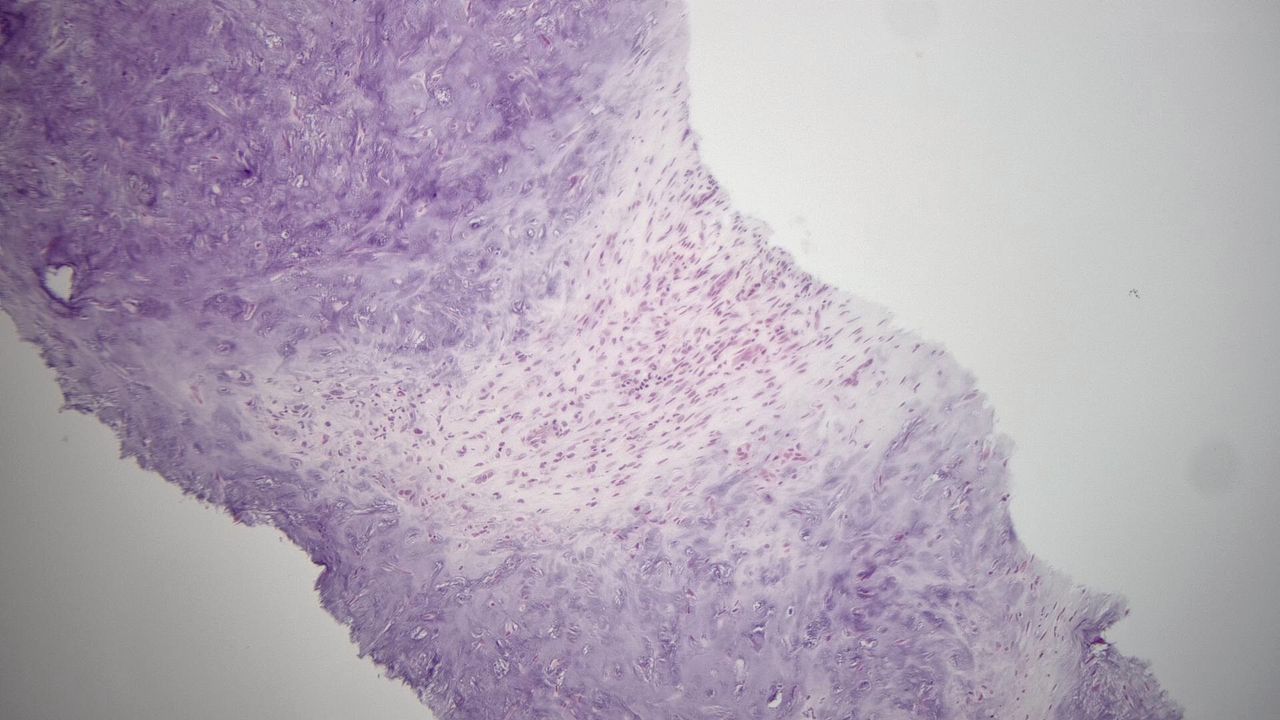
A CT-guided bone biopsy was performed, which showed areas of myxoid/chondroid tissue containing scattered stellate cells with no mitoses or necrosis in keeping with CMF (figure 4). The patient underwent cryotherapy soon after and subsequently reported a significant improvement in her symptoms at follow-up 6 months later.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CT-guided needle core biopsy sample, which shows areas of myxo/chondroid tissue with a zonal architecture and separated by loose fibrous tissue containing a few small multinucleate cells.
Discussion
The occurrence of CMF in the pelvic bones is rare. We conducted a literature review in PubMed by combining the term chondromyxoid fibroma with pelvis, ilium and sacroiliac, and identified several studies relevant to our own, which included 80 cases of pelvic bone CMF with 58 localised to the iliac bones.3 5–21 Of the latter, 17 cases included information on demographics; the median patient age was 36 with a range of 10–68; 8 patients were men and 9 were women. Ten cases provided information on lateralisation and lesion size; six lesions occurred on the left and four on the right; the median lesion diameter was 5.0 cm with a range of 2.1–17.6 cm. The main presenting complaint was one of chronic pain relating to the lower back, buttock, pelvis, lower limb or groin; however, a palpable mass and lower limb weakness were also documented.
The radiological appearance of CMF is non-specific and can vary according to anatomical site. Wu et al reviewed the clinical, radiographic and pathological features of CMF in a series of 278 patients and noted that the most common plain radiographic findings were of an osteolytic lesion with a purely lucent matrix (90%), sharp margins (94%), cortical thinning (90%) and expansion (85%). Other less common findings included a lobulated outline (58%), sclerotic rim (59%) and focal absence of the cortex (50%).5 Overall, the appearance is invariably one of a benign osteolytic lesion.
CT is useful to assess for intralesional calcification, disruption of the cortex and soft tissue extension. While microscopic calcification has been reported on histology in up to 35% of cases, the presence of macroscopic calcification on plain film and/or CT is far less common (2%–15%) and should lead one to include other more common cartilaginous bone tumours within the differential (table 1).1 5 22–24 Interestingly, the incidence of calcification in CMF has been reported as being higher in both older patients and in lesions occurring in the flat bones, which may add to diagnostic uncertainty.5 Pathological fractures relating to CMF are extremely rare (1.6%) and are thought to be the main cause of periosteal reaction, though this is not true for all cases.5 10 Lastly, Wu et al also described soft tissue extension as an uncommon occurrence; however, this observation was based on plain radiographic findings alone and without the use of cross-sectional imaging.5
Common cartilaginous bone tumours and chondromyxoid fibroma1 5 22–24
MRI provides further characterisation and demonstrates the extent of the lesion and its relationship with surrounding structures. The MRI features of CMF were relatively uniform across all studies and consisted of low-to-intermediate signal on T1-weighted sequences, diffuse low signal on T2-weighted sequences and heterogeneous intermediate-to-high signal on T2 fat-saturated sequences.3 In one study, peripheral nodular enhancement was demonstrated in approximately 70% of cases and diffuse heterogeneous or homogeneous enhancement in the other 30%.25 Other studies have described specific MRI features including a low signal intensity rim on all sequences and a lack of or minimal bone or soft tissue oedema as useful in distinguishing CMF from CS; however, such findings appear unreliable and are not commonly used.3
Ultimately histology is required for definitive diagnosis. For the practising histopathologist, the important distinction to be made is between CMF and CS. CMF can be misdiagnosed histologically as a malignant lesion due to the presence of large pleomorphic cells; however, in well-differentiated CS the well-formed hyaline cartilage is usually easily appreciated and the myxoid metachromatic matrix and hypocellular central area of the lobules seen in CMF are usually absent.19 CB also may contain areas of myxoid tissue and spindle cells similar to those seen in CMF; however, other features such as a pericellular ‘chicken wire’ pattern of calcification are not uncommon and pathognomonic for CB.19 Enchondroma may also be included in the histopathological differential diagnosis; however, the presence of mature hyaline cartilage in these tumours is a good differentiating feature.26
Conclusion
This case demonstrates CMF, an already rare bone tumour, in a rare location. The patient’s age and size of the lesion is concordant with descriptions of CMF in more typical locations throughout the body. With regard to pelvic bone CMF, prior studies often describe difficulties in establishing a definitive diagnosis. Peak incidence may occur beyond the accepted third decade of life and lesions may grow to a larger size to fill the pelvic bones. The imaging findings are similar for both pelvic and non-pelvic CMF, yet non-specific overall. Useful differentiating features such as intralesional calcification, while more common in malignant lesions such as CS, can still occur in CMF with higher rates reported in pelvic CMF specifically. Soft tissue extension again is rare but can occur in both CMF and CS. Definitive diagnosis relies on histological sampling; however, the histopathologist must be vigilant while excluding both CS and CB. This paper adds another case to the literature and highlights the need for awareness of CMF in this challenging location and for the integration of imaging and histological findings in order to clinch the diagnosis.
Learning points
Chondromyxoid fibroma (CMF) is a rare, benign bone tumour most commonly located within the metaphyseal region of the long bones, particularly surrounding the knee joint.
Its occurrence in older patients or atypical locations such as the pelvis can lead to diagnostic uncertainty and confusion with malignant lesions such as chondrosarcoma (CS).
Imaging findings are similar for both pelvic and non-pelvic CMF but non-specific across all modalities.
Histological sampling is required for definitive diagnosis; however, the practising histopathologist needs to remain vigilant while excluding both CS and chondroblastoma.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors SA drafted and revised the paper. SL initiated the collaborative project and revised the draft paper. She is the guarantor. AM initiated the collaborative project.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.