Article Text

Abstract
Siponimod is a sphingosine-1-phosphate receptor modulator used as disease-modifying therapy for relapsing-remitting multiple sclerosis similar to Fingolimod which has been known to cause dose dependent fingolimod associated macular oedema (FAME). We report a case of delayed onset bilateral cystoid macular oedema in a patient with stable proliferative diabetic retinopathy who developed cystoid macular oedema in the setting of siponimod (Mayzent; Novartis Pharmaceuticals; Cambridge, Massachusetts, USA) use. As with FAME, cystoid macular oedema resolved in the patient’s eyes with drug cessation and adjunctive topical anti-inflammatory therapy. We highlight unique fluorescein angiographic findings within this class of drugs as well as the clinical challenge posed by comorbid diabetic and inflammatory ophthalmic pathology.
- Drugs: CNS (not psychiatric)
- Retina
- Macula
- Unwanted effects / adverse reactions
- Multiple sclerosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The advent of multiple new therapeutic modalities and targets for multiple sclerosis (MS) has greatly impacted patient quality of life. However, like any therapy, benefits must be weighed against the risks of adverse events associated with such therapies.
Here, we describe bilateral cystoid macular oedema in the setting of recent initiation of siponimod in a patient with diabetes with proliferative diabetic retinopathy. We also further outline the findings of intravenous fluorescein angiography (IVFA) in this class of medications.
Case presentation
A woman in her 50s with a history of MS, type 2 diabetes mellitus, antiphospholipid antibody syndrome and chronic renal failure presented to the ophthalmology clinic with a 6-day history of blurry vision in the left eye.
On presentation, her best-corrected visual acuity was count fingers at 2 ft in the right eye (OD) and 20/60 in the left eye (OS) with no improvement on pinholing. Compared with exams in the prior year, her visual acuity had decreased from 20/40 to 20/60 in the left eye. The right eye’s vision remained stable at count fingers vision at 2 ft. Intraocular pressure was 16 mm Hg in both eyes (OU). Anterior segment examination was unremarkable except for known moderate nuclear sclerotic cataracts. Posterior segment examination revealed known bilateral optic nerve head pallor with a cup-to-disc ratio of 0.3 in both eyes with 360° of pan-retinal photocoagulation scars.
Her medical history was significant for an episode of non-steroid responsive optic neuritis in the right eye 27 years prior and another episode, 2 years after the initial episode, in the left eye that did improve with intravenous steroids. Six months prior to presentation, she was diagnosed with relapsing remitting MS on MRI following presentation for gait disturbance, right sided weakness and slurred speech secondary to a left mid pontine lesion. She was started on siponimod (Mayzent; Novartis Pharmaceuticals; Cambridge, Massachusetts, USA) as disease-modifying therapy for her MS 1 month after diagnosis. She presented 5 months after initiation of siponimod.
In addition, she had an ocular history of bilateral proliferative diabetic retinopathy without macular oedema. She had been followed by ophthalmology for 15 years for diabetic retinopathy treated with pan-retinal photocoagulation of both eyes (OU). During her course, she had never had documented diabetic macular oedema. Her last haemoglobin A1c about 1 month prior to presentation was 10.2.
Investigations
Optical coherence tomography (OCT) OS on presentation revealed intraretinal and subretinal fluid in the fovea. Poor signal precluded adequate comparative imaging of the right eye at that time.
Eight days later, her clinical examination was unchanged from prior. Repeat OCT of the macula demonstrated worsening bilateral cystoid macular oedema in both eyes (figure 1A,B). IVFA demonstrated late petaloid macular leakage and late staining of the optic discs (figure 2A,B).
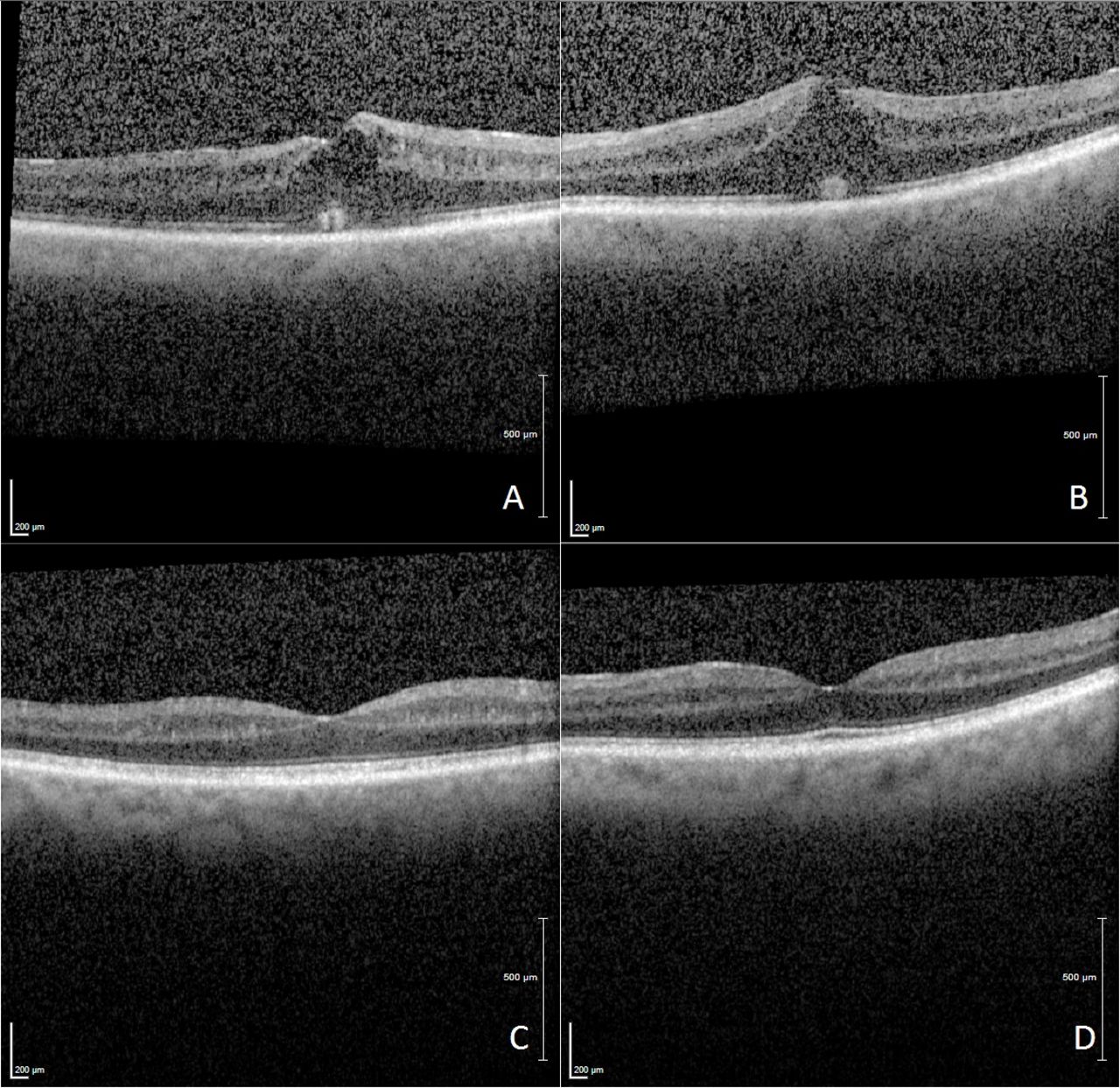
Macular OCT of the (A) right and (B) left eye at first follow up visit 1 week after presentation showing bilateral intraretinal and subretinal fluid and worsening distortion of foveal contour followed by resolution of intraretinal fluid in the (C) right and (D) left eye at the third follow-up visit (2 months from presentation). OCT, optical coherence tomography.

{kind=link}
{kind=link}
Late fluorescein angiography (FA) of the (A) right and (B) left eye on 1-week follow-up after initial presentation demonstrating petaloid leakage and optic nerve head staining. FA 16 weeks after discontinuing siponimod in (C) right and (D) left eye with resolution of leakage and staining.
Differential diagnosis
Based on the patient’s significant history of proliferative diabetic retinopathy and treatment of MS, the initial presentation was concerning for diabetic macular oedema versus macular oedema associated with drugs used for disease modifying treatment of MS. Findings on OCT imaging and IVFA were more consistent with a cystoid macular oedema pattern given late petaloid macular leakage and disc staining. The differential besides siponimod-related cystoid macular oedema for disc staining included breakthrough optic neuritis.
Treatment
The patient was started on topical ketorolac 0.5% and prednisolone acetate 1% twice daily in the left eye and scheduled to follow up in a week with a retina specialist.
After follow-up, the patient’s ketorolac and prednisolone acetate drops were increased to four times a day in both eyes.
Given concern for possible drug-related cystoid macular oedema, neurology was consulted to discuss a change to a different agent. The siponimod was discontinued with plans to start a different agent for control of MS.
Outcome and follow-up
On follow-up at 3 weeks after initial presentation and after discontinuation of siponimod, the patient noted subjective improvement in her vision corresponding with improvement on OCT imaging. However, her best-corrected visual acuity was objectively noted to be unchanged. She was started on a taper of her eye-drop regiment in both eyes over the next 3 weeks.
On follow-up at 2 months after initial presentation, the patient had completed her eye-drop taper. Her vision was documented as having improved to 20/25 in the left eye with complete resolution of the macular oedema in both eyes (figure 1C,D and figure 2C,D).
Over the subsequent month, she was started by neurology on dimethyl fumarate for management of her MS and no recurrence of cystoid macular oedema was noted at over 3 months from initial presentation.
Discussion
Fingolimod is a disease-modifying therapy for relapsing-remitting MS that acts to modulate the sphingosine-1-phosphate receptor with known dose dependent fingolimod associated macular oedema (FAME).1–3 The drug acts to decrease lymphocyte release into systemic circulation from peripheral lymphoid organs.2 4 It is thought that by interacting with the endothelial S1P receptor, fingolimod induces vascular permeability.5 6
The Food and Drug Administration recommends baseline ophthalmological examination before initiating therapy with fingolimod and repeat studies at 3–4 months with extended follow-up thereafter if without FAME.7
Cystoid macular oedema in these cases typically resolves with drug cessation, but time to resolution can vary.8 Other therapeutic options have been reported with variable success and include systemic carbonic anhydrase inhibitors, topical non-steroidal anti-inflammatory drugs (NSAIDs) and even oral steroids.8–10
Newer agents in the same class such as siponimod have traditionally been thought not to be associated with the same risk of ME based on the dose-blinded extension of the phase 2 BOLD trial which demonstrated no cases of macular oedema.11 12 However, in the phase 2 BOLD trial, macular oedema was reported in one patient with a history of uveitis on the highest dose of siponimod (10 mg) and one patient with optic neuritis on 0.5 mg of siponimod.13 The phase 3 EXPAND trial found a higher rate of macular oedema (2%) compared with placebo (<1%).3 14 It should be noted that the EXPAND trial excluded patients with ongoing macular oedema and uncontrolled diabetics from the trial.14
A case report by Rettler and Gratton demonstrated a similarly delayed presentation of macular oedema 3 months after initiation of siponimod in a patient with MS that resolved with drug cessation and topical anti-inflammatory therapy as well.15 Our case demonstrates a 5-month delay between drug initiation and symptom onset. We agree with Rettler and Gratton’s recommendation for baseline ophthalmic examination and counselling of patients on siponimod as well as monitoring given the potential lag of symptom onset following commencement.15
Our case illustrates unique fluorescein angiographic findings in siponimod that may be representative of the class of S1P receptor modulators. Soliman et al demonstrated fluorescein angiographic findings consisting of petaloid cystoid macular oedema, perivascular leakage from peripheral vessels, hyperfluorescence of dilated peripapillary vascular frond and optic nerve head staining associated with fingolimod in FAME.8 We report similar angiographic findings to Soliman et al in a patient on siponimod including petaloid leakage and optic nerve staining.8 To our knowledge, these angiographic findings have not been documented in Siponimod related macular oedema as they have in FAME. Cognizance of these angiographic characteristics in S1P receptor modulators may hasten diagnosis and prevent unnecessary treatment of cystoid macular oedema.
This case shows how history of diabetic retinopathy may complicate and delay identification of other aetiologies of macular oedema that may initially be attributed to diabetes. Although the mechanism is not established, the compromised blood retinal barrier and blood ocular barrier in patients with diabetic macular oedema and uveitis, respectively, may contribute to the higher risk of macular oedema with siponimod use in these patients.1 16 17 Patients with diabetic retinopathy without history of macular oedema may also be at risk of developing macular oedema in the setting of subclinical microvascular changes. Optic neuritis and other inflammatory optic neuropathies can also demonstrate disc staining and filling delays on IVFA.18 Comorbid inflammatory disorders causing macular oedema in the setting of possible concurrent optic neuritis may present similarly to this case on IVFA. Of note, varicella zoster virus reactivation which may represent one form of optic neuritis was also noted in secondary analysis of the EXPAND trial.3 As such, we recommend that clinicians consider these factors in patients who may be at higher risk of developing macular oedema with siponimod use. The prescribing information for siponimod now includes recommendations for baseline ophthalmological exam prior to initiating siponimod and reassessment if any visual changes develop with caution that those with history of diabetes and uveitis are at higher risk of developing macular oedema. Thus, it is important to closely monitor such patients when discontinuing disease modifying therapy suspected of causing macular oedema. We posit the necessity of extension of baseline counselling and ophthalmic evaluation of patients on S1P receptor modulators as a drug class, particularly in patients with comorbid diabetes mellitus and history of uveitis.
In conclusion, we report a case of bilateral cystoid macular oedema in the setting of siponimod (Mayzent; Novartis Pharmaceuticals) use in a patient with stable proliferative diabetic retinopathy without documented history of macular oedema. The aetiology of macular oedema can be masked by confounding ocular comorbidities such as diabetic retinopathy and was successfully managed with discontinuation of therapy and with topical anti-inflammatory drops.
Learning points
Siponimod, a selective sphingosine-1-phosphate (S1P) receptor modulator for treatment of relapsing-remitting multiple sclerosis, can be associated with macular oedema in patients with diabetic retinopathy without history of macular oedema.
Intravenous fluorescein angiography for S1P receptor modulators such as fingolimod and siponimod demonstrates both petaloid macular leakage and optic disc staining.
Identifying siponimod associated macular oedema can present a diagnostic challenge in patients with diabetic retinopathy or other inflammatory ophthalmic conditions and is important for disease management.
Macular oedema associated with siponimod may have a delayed symptomatic presentation by months after drug initiation.
Recommended baseline ophthalmological examination and counselling prior to initiating fingolimod as well as monitoring should be extended to S1P receptor modulators such as siponimod as a class of drugs, particularly in patients with concomitant diabetes or uveitis.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @ophthalmaton
Contributors WFF: provided the primary edits and creation of the manuscript. CC: assisted in edits of the primary manuscript and helped collate imaging information and captions to generate figures. MA: assisted in manuscript edits and obtaining consent from the patient. MP: was clinically responsible for the patient and oversaw and guided the creation of the manuscript along with providing feedback for edits of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.