Article Text

Abstract
We report the 4-year postoperative outcome of a child with Manner Type I aplasia of the anterior cruciate ligament (ACL) in her left knee and severe genu valgum. The child was experiencing pain, reduced mobility, and frequent left knee locking and instability. The patient was successfully treated with hemiepiphysiodesis (guided growth procedure) of the left knee joint to treat genu valgum deformity using 8-plates, resulting in improvement of knee stability. This spared her major ligament reconstruction of the knee to treat the aplastic ACL, and the patient was able to fully participate in physical activities with peers with no symptoms.
- Developmental paediatrocs
- Knee laxity
- Paediatric Surgery
- Orthopaedic and trauma surgery
Statistics from Altmetric.com
Description
Congenital absence of the cruciate ligaments is a rare condition that was first reported by Giorgi in 1956 and has a prevalence of 0.0017 per 1000 live births.1 Patients are often asymptomatic and treated with physiotherapy and analgesia.2 With symptoms of progressive pain and instability, ligament reconstruction is often undertaken.3 This procedure aims to eliminate symptoms and prevent osteoarthritis from developing in adulthood, but as yet, there is no documented evidence that osteoarthritis occurs without reconstruction.4 5
We report the 4-year postoperative outcome of a child with a background of Pierre Robin sequence, who was found to have Manner Type I aplasia of the anterior cruciate ligament (ACL) and normal posterior cruciate ligament in her left knee, and severe genu valgum (knocked knee deformity).6 The patient was successfully treated with hemiepiphysiodesis (guided growth procedure) of the left knee joint to treat genu valgum deformity using 8-plates, resulting in improvement of knee stability, sparing her major ligament reconstruction of the knee.
The child presented in the clinic with a 5-year history of pain, reduced mobility and left knee locking. She had frequent instability of her knee, which gave way particularly when performing twisting activities. These symptoms were previously thought to be due to gait pattern as the child had left flexible genu valgum deformity with knee hyperextension and signs of locking when standing at 25° of flexion. By this point, management with ankle-foot orthosis was no longer sufficient, and a wheelchair was required after ten minutes of walking.
At the time of presentation in the paediatric orthopaedic clinic, on clinical examination the child demonstrated positive left knee anterior draw and pivot shift tests, both clinical tests indicating knee instability due to ACL deficiency. The patient experienced no symptoms of pain or instability on the right knee, and on examination, the right knee felt stable with negative anterior draw and pivot shift tests. Long view radiographs demonstrated a mechanical axis passing lateral to the midline of the tibia plateau (Paley Zone II), indicating moderate genu valgum (figures 1 and 2).7 The right lower limb alignment was normal.

Long leg view radiograph of the patient indicating genu valgum of the left knee (knocked knee deformity). Mechanical axis (yellow line) connecting centre of the left hip with centre of the left ankle is passing laterally to centre of the left knee joint.

A zoomed image of the left knee demonstrates the preoperative moderate genu valgum deformity showing the mechanical axis (yellow line) passing through the lateral Paley Zone II (division of the lateral knee compartment in three zones—red lines).
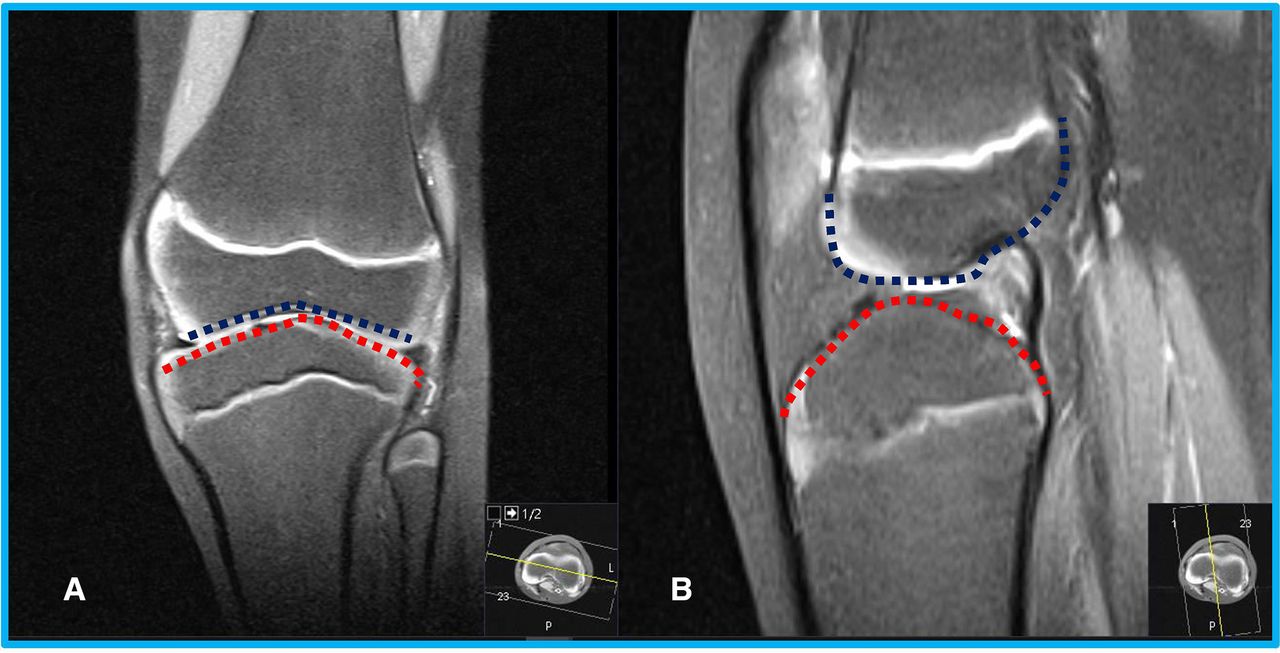
An MRI was requested, and congenital absence of ACL was diagnosed in the left knee (figure 3). The proximal tibia epiphysis appears convex on the coronal view of the MRI scan with a medial and lateral tilt and a peak midpoint; the corresponding distal femur surface appears congruent with a concave contour (figure 4). In contrast, on the sagittal view, there is a posterior and anterior tilt and a peak midpoint of the proximal tibia epiphysis, and an incongruent corresponding distal femoral surface (figure 4).

A sagittal view of an MRI scan of the patient’s left knee showing congenital absence of the anterior cruciate ligament (yellow arrow).
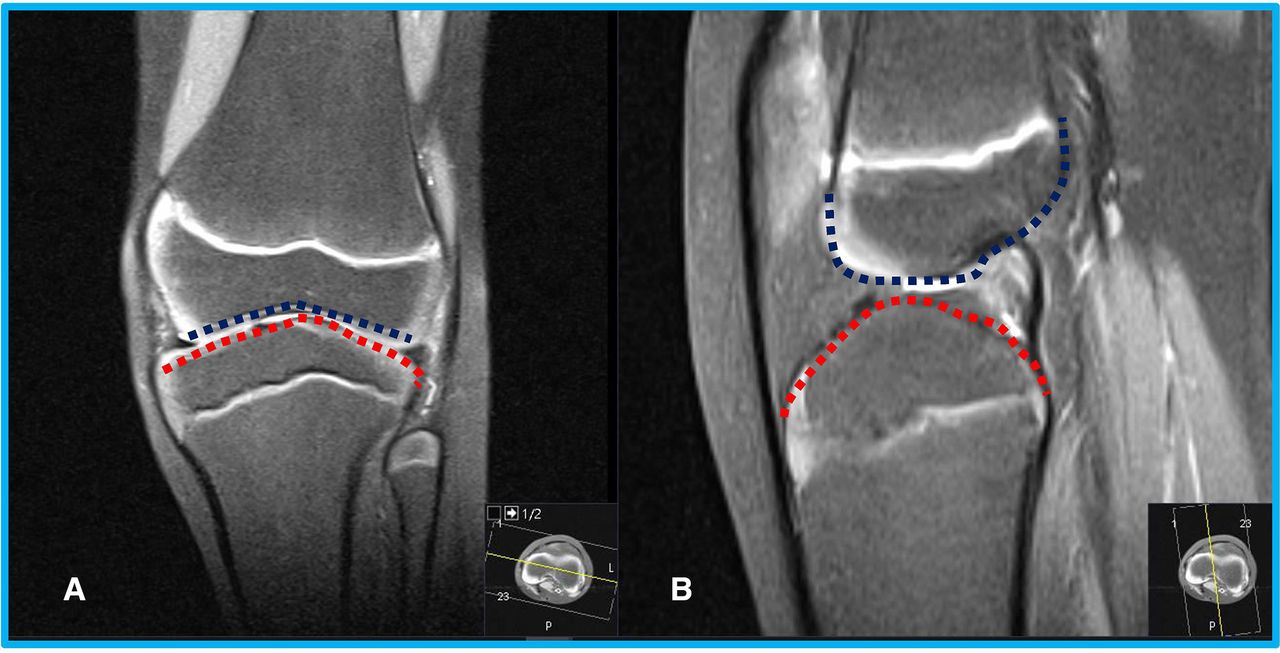
Coronal and sagittal view MRI scans of the patient’s left knee. The proximal tibia epiphysis appears convex on the coronal view (A) with a medial and lateral tilt and a peak midpoint (red dotted line), while the corresponding distal femur surface appears congruent with a concave contour (blue dotted line). On the sagittal view (A), there is a posterior and anterior tilt and a peak midpoint of the proximal tibia epiphysis (red dotted line) with an incongruent corresponding distal femoral surface (blue dotted line).
This demonstrated incongruency of the dysplastic knee articular surfaces on the sagittal view of the MRI, which was thought to be contributing to the patient’s clinical anterior instability symptoms, together with the congenital ACL absence. The articular dysplasia can also explain the signs of knee locking when standing at 25° of flexion.
After discussion of surgical options with the family and the senior surgeon (MK), it was decided to correct the lower limb malalignment via minimally invasive temporary hemiepiphysiodesis (guided growth) of the left knee using 8-plates. The principle of the ‘guided growth’ procedure is that if low-profile plates (such as the so-called ‘8-plates’) with the relevant screws are inserted in the convex side of a lower limb deformity then the growth on that side of the knee joint is temporarily slowed down, while the concave side of the knee deformity will continue to grow and gradually the alignment of the lower limb will be re-established. It was thought that reconstruction of the congenitally absent ACL should only be considered if symptoms continued after lower limb alignment correction, otherwise the reconstruction might be compromised in the presence of a structural limb alignment deformity. It was also assumed that symptoms would improve after guided growth.
The 8-plates and screws were inserted at the distal medial femur and proximal medial tibia, slowing down temporarily the longitudinal growth on the medial aspect of the knee and allowing further growth on the lateral aspect of the knee (figure 5). Successful manipulation of the growth plates above and below the knee joint in combination with skeletal growth should result in asymmetrical growth of lower femur and upper tibia and subsequent correction of the knocked knee deformity. This is an orthopaedic procedure than can be performed as a day case and allows full weight bearing after surgery. The guided growth procedure was undertaken on our patient a few months after her presentation in the paediatric orthopaedic clinic.

Long leg view, postoperative radiograph of the patient demonstrating insertion of the 8-plates in the distal medial femur and proximal medial tibia (double red arrows) at the age of 11 years.
Two years following the guided growth surgery to her left knee, the child had a fall on her right hip and sustained a proximal right femoral fracture which was treated with internal fixation at the local hospital. This fall and the subsequent additional orthopaedic procedure did not influence the outcome of the guided growth to the left knee but has resulted into a genu valgum deformity of the right knee.
The child was followed regularly, and four years following the surgery the metalwork was removed with the intention of leaving a mild left genu varum overcorrection. This was done to prevent ‘rebound’ recurrence of the deformity with further growth (figures 6 and 7).

Long leg view radiograph of the patient at 15 years of age showing removal of the metalwork (double white arrows) and resolved genu valgum of the left knee, whereby the mechanical axis (yellow line) passes just medial to the midline of the left knee. The same radiograph also demonstrates the internal fixation used to treat the right hip fracture the patent sustained 2 years prior to the removal of metalwork from the left knee (red arrow).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A magnified image of the left knee demonstrates the postoperative radiograph with the slightly overcorrected left lower limb alignment and the mechanical axis (yellow line) passing through the medial Paley Zone I. The medial knee compartment is divided into three zones (blue lines).
The guided growth procedure changed the biomechanical relation of both dysplastic articular surfaces of the left knee. This resulted in improvement of objective and subjective knee stability in the absence of an ACL, and the patient was able to fully participate in physical activities with peers with no symptoms.
The patient and her mother did not wish to consider surgical intervention for the resulting right genu valgum deformity and the minimum apparent leg length discrepancy of less than 1 cm following the internal fixation of the right proximal femoral fracture.
Patient’s perspective
A comment from the patient’s parent: The operation went extremely well, so much so that [the patient] was up on [their] feet the next day and walking around the ward. [Their] pain level was minimal. It has done wonders for [their] mobility; [they] now walk around rather than using [their] wheelchair and [they] don’t get the pain in [their] knee that [they] used to get.
Learning points
Congenital absence of the cruciate ligaments is rare; absence of the anterior cruciate ligament (ACL) is more common than absence of the posterior cruciate ligament and is either found in isolation or in association with other lower limb abnormalities, usually limb dysplasia and patella dislocation.
In rare conditions such as ACL congenital absence with associated structural deformities, a more straightforward and routine-guided growth procedure can be undertaken compared with a complex and infrequently performed reconstruction of an absent ligament.
Minimally invasive guided growth procedure using 8-plates was performed on our patient to realign the lower limb which resolved the knee pain as well as the instability.
Ethics statements
Patient consent for publication
Footnotes
Twitter @thomasllewis
Contributors MK performed both surgeries on the patient and conceived of the idea of writing a case report. TLL assisted MK in the second surgery of removing the 8-plates. PM wrote up the case report for MK, and it was then edited by TLL and MK.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.