Article Text

Statistics from Altmetric.com
Description
A South Asian woman in her 60s, presented with complaints of blurring of vision in her right eye for 10 days. She was a known case of adenocarcinoma of the lungs with brain metastasis. Her recent positron emission tomography scan showed hepatic metastasis and regressing lobulated mass in the lungs but no ocular involvement. She had received radiotherapy and chemotherapy in past and was recently started on immunotherapy with atezolizumab, bevacizumab and paclitaxel. The best corrected visual acuity in the right eye was 20/800 and the left eye was 20/20. Intraocular pressure in both eyes was 12 mm Hg. Left eye examination was within normal limits with visually insignificant age-related cataract. Right eye anterior segment examination was normal, but fundus examination showed large vitreous cells, optic disc infiltrates, pseudosheathing and a boat-shaped lesion inferiorly in the vitreous (figure 1A). Optical coherence tomography revealed preretinal deposits and large cells in the vitreous (figure 1B).
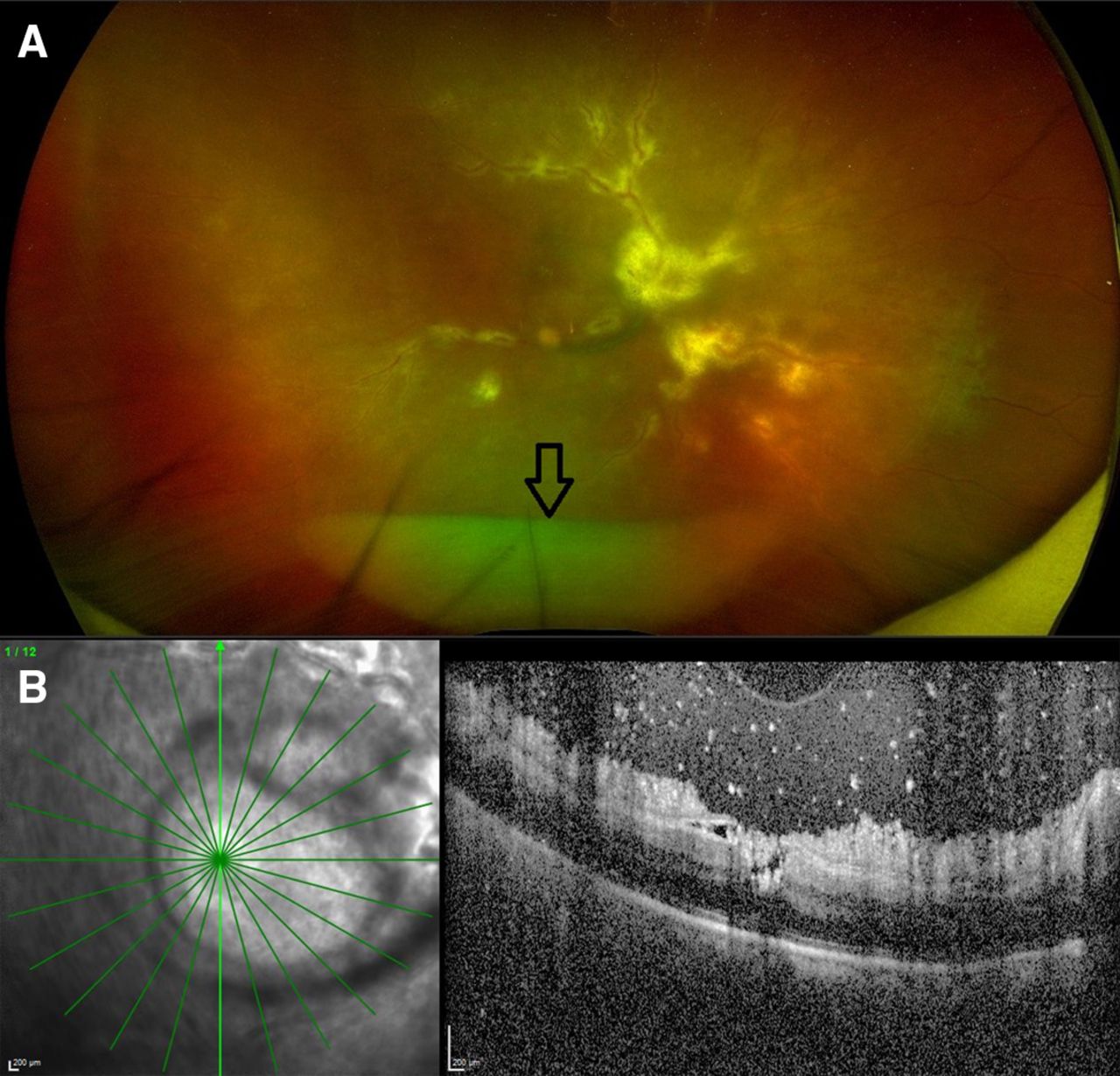
(A) Widefield fundus photograph shows whitish-yellow optic disc infiltrates, a ‘candle wax dripping’ like pseudosheathing and a peculiar ‘boat-shaped’ yellowish-white lesion inferiorly in the vitreous (arrow). (B) Optical coherence tomography shows a preretinal sheet of amorphous material.
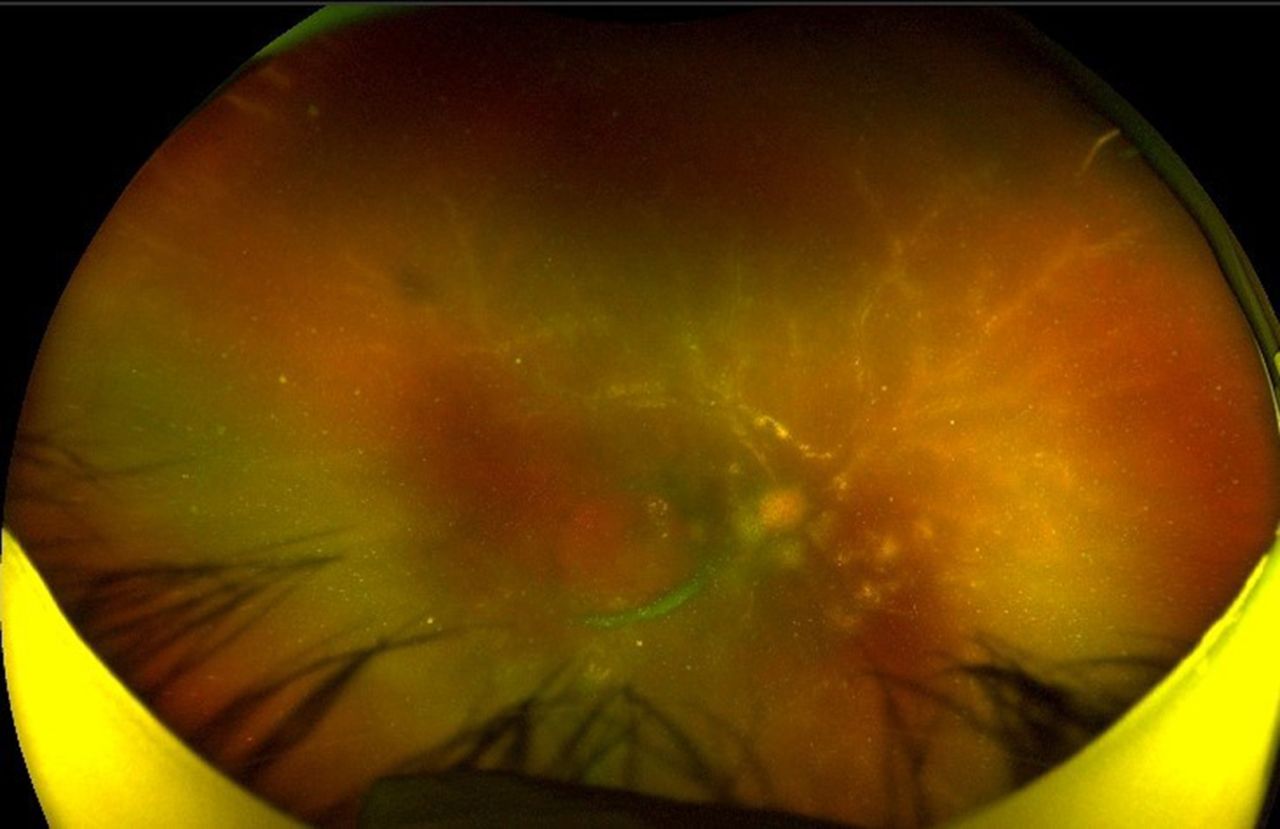
A diagnosis of masquerade syndrome with ocular metastasis was made and a diagnostic vitreous tap was advised which the patient declined. The patient was restarted on radiotherapy to the head by her oncologist and immunotherapy was continued. After 4 months remarkable improvement was noted in the fundus picture but without any visual gain. The boat-shaped vitreous lesion was dissolving, the disc infiltrates and the pseudosheathing of retinal vessels showed signs of resolution (figure 2).

{kind=link}
{kind=link}
Widefield fundus photograph shows resolving pseudosheathing and disc infiltrates.
Posterior hypopyon in endophthalmitis,1 pseudohypopyon in the anterior chamber in systemic malignancies2 and boat-shaped dehaemoglobinised preretinal haemorrhages3 are well-recognised ocular findings. The novel finding of boat-shaped cellular aggregates of metastasising adenocarcinoma in the vitreous cavity as seen in our case can be confused with infectious posterior hypopyon and long-standing vitreous haemorrhage. The absence of inflammatory signs in the anterior segment, absence of retinal haemorrhages or neovascularisation, and presence of optic disc infiltrates and the pseudosheathing suggested ocular metastasis which was further confirmed by the favourable therapeutic response to the radiotherapy and continuation of immunotherapy in our case.
Learning points
Apart from infections and dehaemoglobinised preretinal boat-shaped haemorrhage posterior pseudohypopyon can be a feature of metastatic adenocarcinoma.
Disc infiltration with adenocarcinoma may lead to permanent loss of vision.
Ethics statements
Patient consent for publication
Footnotes
Contributors Study planning, conduct, reporting, conception and design, acquisition of data or analysis and interpretation of data: AKa. Study conduct, reporting and design, analysis and interpretation of data: AKh. Study conduct, reporting and conception: SS. Manuscript editing and final approval: PM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.