Article Text

Statistics from Altmetric.com
Description
A previously healthy 29-year-old man presented with an anterior chest wall asymmetry, which according to the patient, developed insidiously and persisted with no obstructive symptoms. There was additionally significant unintentional weight loss of 5 kg over the past 6 months. On further questioning, the patient mentioned that a blood test performed for routine medical check-up revealed iron-deficiency anaemia features, and he was given haematinics which he defaulted. No inciting trauma, fever, drug allergy or travel history was unveiled. Additionally, no signs and symptoms of anaemia were demonstrated. On examination, the patient appeared comfortable under room air, with no pallor. Non-erythematous, generalised facial puffiness was noted with no palpable neck swelling. The anterior chest wall appeared asymmetric, which was prominent over the right anterior chest wall. Pemberton test result was negative (figure 1). Besides features of hypochromic microcytic anaemia, other routine blood investigations along with electrolytes were within the normal range. A chest radiograph revealed widening of the mediastinum with no abnormal lucency (figure 2).

Asymetrical chest wall with negative Pamberton’s sign.
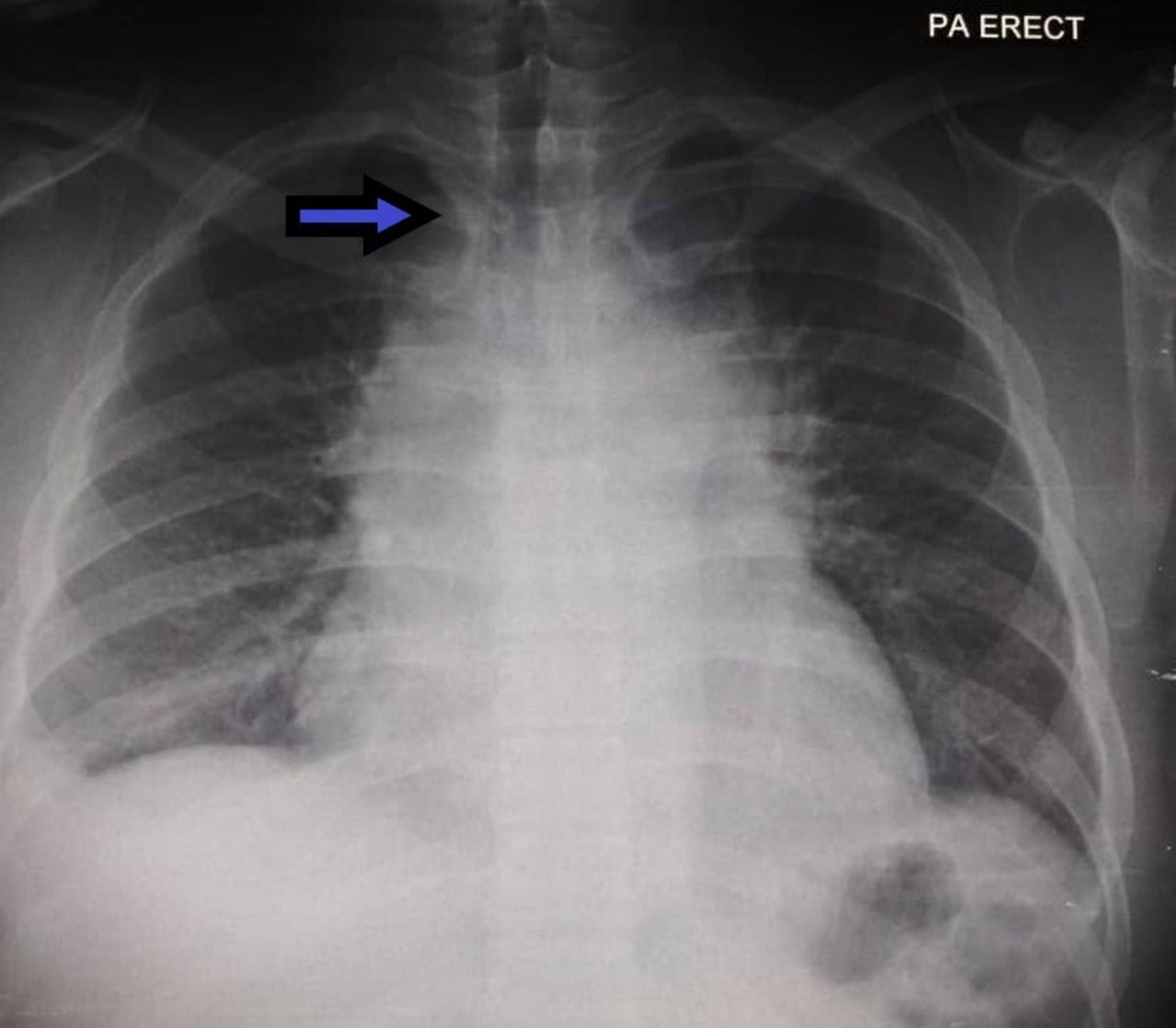
Chest X-ray with widening of mediastinum.
The patient subsequently underwent a CT of the thorax, which revealed an enhancing anterior mediastinal mass extending from sternal manubrium to the xiphoid process measuring 9.0×12×14 cm (figure 3). A histopathological examination of a CT-guided biopsy revealed neoplastic lymphoid cells, which appeared to be mononuclear Hodgkin’s and multinucleated Reed-Sternberg cells, and prominent nucleoli with frequent mitotic figures. Immunohistochemistry staining is positive for CD79a, PAX5 and CD30, which was consistent with classical Hodgkin’s lymphoma (HL). The patient was referred to the haematology unit, and chemotherapy was started. The patient responded positively to prompt chemotherapy.

{kind=link}
{kind=link}
{kind=link}
CT thorax revealing anterior mediastinal mass.
Primary mediastinal malignancy is a rare entity with vague clinical presentations. Lymphoma stands as the most common malignancy of the mediastinum, notably HL. HL is a haematological malignancy that shows bimodal distribution of age, exhibiting peaks at adolescence and after 50 years.1 Early intrathoracic involvement has been documented in more than 80% of cases especially involving the anterior mediastinal as well as the paratracheal nodes.2 Nearly 50% of patients with primary mediastinal HL remains oblivious on presentation as it is oftentimes discovered incidentally. However, patients may complain of vague symptoms such as chest pain, fatigue, dyspnoea or cough. B-symptoms (fever, drenching night sweats and significant weight loss) have been classically linked to HL in only 30% of patients, whereas itchiness is found nearly in 15% of patients.3 Interestingly, Pel-Ebstein fever, although linked to HL, is also non-specific.3 Superior vena cava syndrome is uncommonly seen, which can be elicited by the Pemberton’s sign.3
First described by Dr Hugh Pemberton in 1946, Pemberton’s sign is described by facial redness and venous engorgement on bilateral arm elevation which occurs due to clavicular movement resulting in a ‘nutcracker’ effect which compresses major venous structures. Pemberton’s sign is reported to be a quick manoeuvre to diagnose superior vena cava syndrome from all aetiologies.4
Laboratory investigations that may favour lymphoma diagnosis include leucocytosis, absolute neutrophilia or eosinophilia, lymphopenia, which can be accompanied by microcytic hypochromic anaemia, and elevated erythrocyte sedimentation rate and lactate dehydrogenase, which correlates with advanced disease.3
A simple plain posterior-anterior radiograph may reveal a widened mediastinum as in our patient. Additionally, primary mediastinal HL appears with a radiopaque mass with smooth or lobulated borders. A lateral view radiograph can verify the localisation of the tumour, which can be either anterior or middle mediastinal. Imaging features of anterior mediastinal mass include multiple, homogeneous soft-tissue mass, although heterogeneous features with low attenuation due to necrosis, haemorrhage or cyst formation can be seldom noted.5
Asymmetric anterior chest wall points to the diagnosis of amazia and amastia. In our patient, the presence of iron-deficiency anaemia with significant weight loss accompanying asymmetric chest wall points towards a more serious pathology.
Gold standard treatment for HL remains a combination of chemotherapy and radiotherapy to the involved site, which has an overall good prognosis, especially in Stages I and II. Various chemotherapy protocols include ABVD (Adriamycin, bleomycin, vincristine and doxorubicin), Stanford V regime (doxorubicin, vinblastine, mechlorethamine, vincristine, bleomycin, prednisolone), escalated BEACOPP (bleomycin, etoposide, Adriamycin, cyclophosphamide, Oncovin, procarbazine, prednisolone) with involved-site radiotherapy (ISRT).6
Learning points
Atypical presentation such as asymmetrical anterior chest wall ought to be investigated instantly.
Simple investigation such as chest radiography may reveal the presence of mass or widening of the mediastinum.
Unexplained abnormal results of routine blood investigation such as anaemia, in addition to unexplained weight loss, should be investigated thoroughly.
Ethics statements
Patient consent for publication
Footnotes
Contributors JS: Drafting, writing, literature review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.