Article Text

Statistics from Altmetric.com
Description
Even though there are few case reports of multidrug-resistant burkholderia causing various infections in immunocompromised individuals, hepatobronchial fistula due to burkholderia is not reported.1–3
A 58-year-old man with no known comorbidities presented with a history of low-grade continuous fever and right-sided abdominal pain for 1 month. He had received tablet paracetamol prescribed by a general practitioner. But his symptoms did not subside, and he had increased fatigue, so he came to the hospital. On general examination, heart rate was 94/min, blood pressure was 134/78 mm Hg and temperature was 39°C. Cardiac, pulmonary and abdominal examinations revealed no abnormality. Laboratory tests were remarkable for a leucocytosis (15 080 cells/mm3), total bilirubin 2.6 mg/dL, alanine transferase 180 U/L, aspartate transferase 72 U/L. Chest X-ray showed an elevated right hemidiaphragm. The patient was admitted and treated with fluids, and empiric antibiotic therapy with piperacillin-tazobactam was started. Baseline investigations and blood cultures were taken.
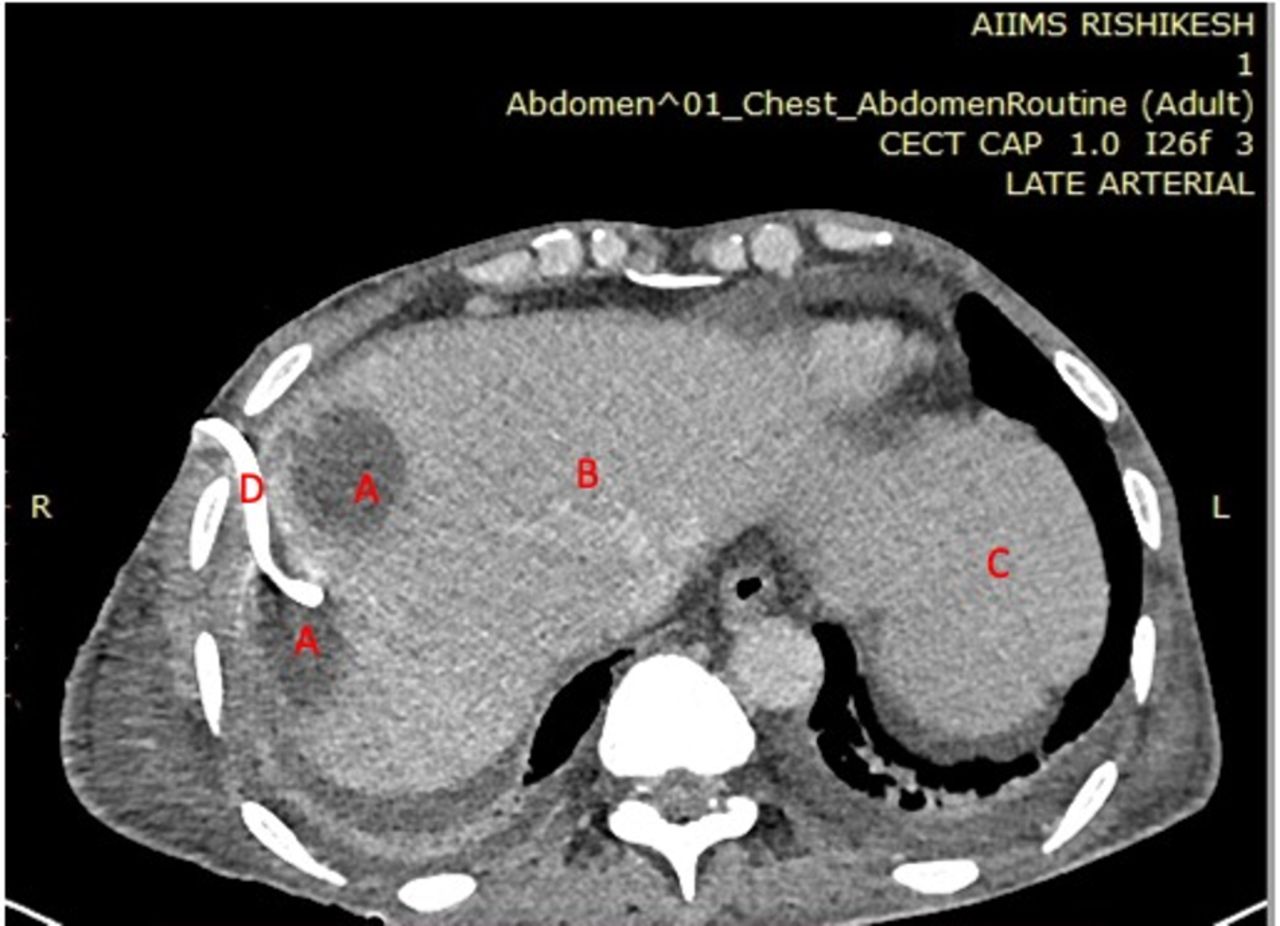
An abdominal ultrasound (US) revealed two hypodense collections (3.5 cm and 4 cm diameter) in the right lobe of the liver. Subsequently, contrast-enhanced CT (figure 1) showed few hypodense collections in both lobes of the liver for which percutaneous drainage was placed, yielding 80 cc of purulent fluid. Entamoeba histolytica serology was negative. On analysis of the fluid,cartridge-based nucleic acid amplification test for tuberculosis and malignant cells were negative. Pus culture from the aspirate subsequently grew multidrug-resistant burkholderia cepacia. Antibiotics were broadened to high intravenous dose-extended meropenem infusion.
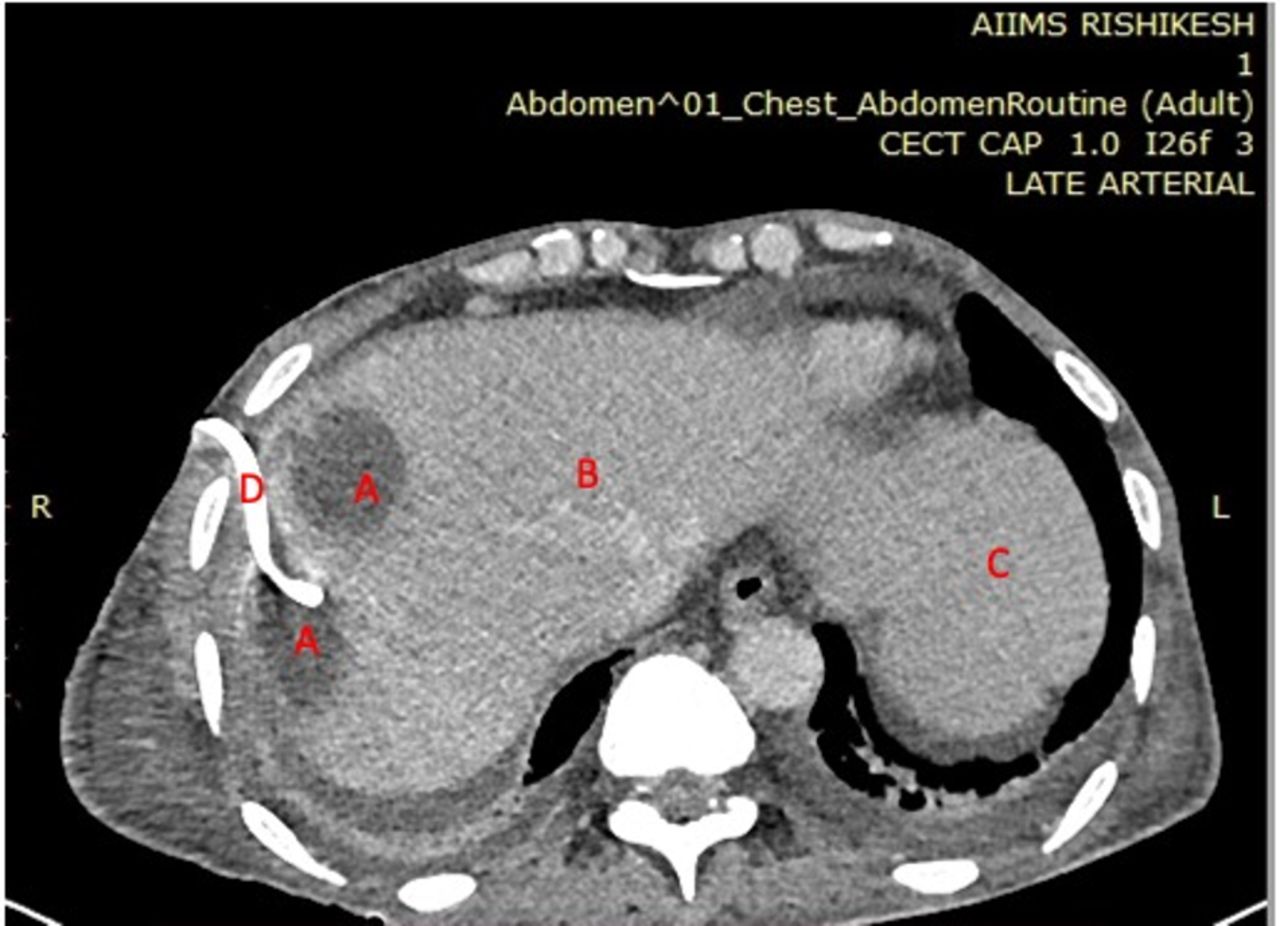
CT scan showing liver abscesses (A—abscess, B—liver, C—stomach, D—drain).
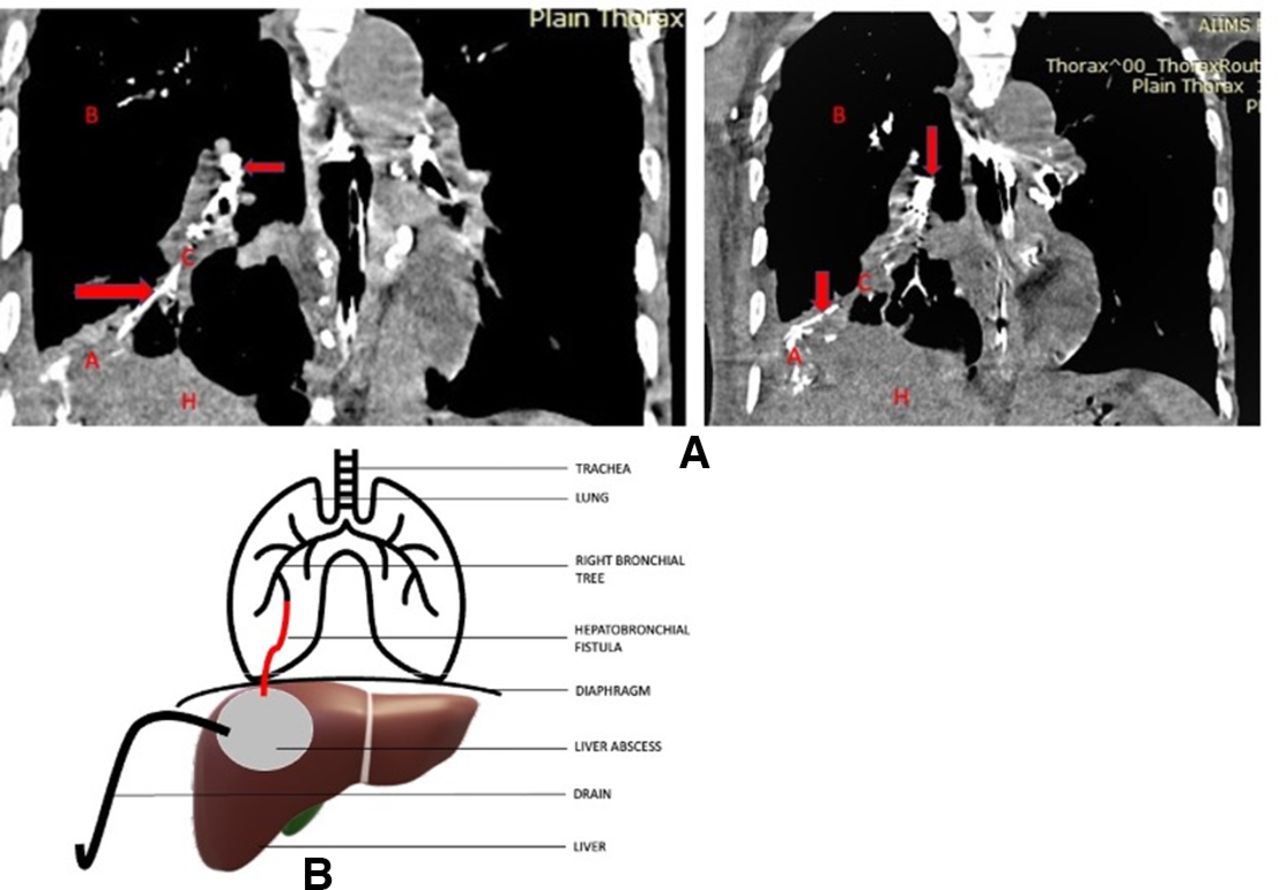
On day 8 of the hospital stay, he developed a dry cough, shortness of breath and a metallic taste in the mouth. We observed that lavage of the abscess caused cough with purulent discharge. Clinical suspicion of the hepatobronchial fistula was made. CT chest and abdomen were done after instillation of contrast through the drain, which revealed a fistulous tract between the liver abscess and the bronchus (figure 2). Hepatic drain decompression was done, and injection tigecycline was added. Over the next 10 days, the drain output gradually decreased. Follow-up CT after 1 month showed resolution of abscess and fistula.

{kind=link}
{kind=link}
(A) Postcontrast CT after instillation of dye through the drain showing hepatobronchial fistula (red arrows), A—abscess, B—lung, C—hepatobronchial fistula, H—liver). (B) Line diagram of hepatobronchial fistula. ***Created by author using Microsoft PowerPoint online 3D models. Permission to reuse.
Common causes of fistulation, investigations of fistula, priorities in treatment and factors in fistula healing are listed below (boxes 1–4).
Common causes of fistulation
Congenital.
Hepatic hydatid cysts.
Amoebic liver abscesses.
Pyogenic liver abscesses.
Biliary tract lithiasis.
Liver trauma.
Surgical complications.
Investigations of fistula
Chest X-ray after instillation of water-soluble contrast material in the hepatic drain tube.
CT abdomen and thorax.
US abdomen.
Endoscopic retrograde cholangiopancreatography.
Percutaneous transhepatic cholangiography.
MRI.
Hepatobiliary iminodiacetic acid scan.
Priorities in treatment
Antibiotics.
Conservative approach (spontaneous closure).
Minimally invasive surgery (percutaneous drainage and decompression of hepatic abscesses).
Radical surgery (lung decortication and diaphragm repair, liver wedge resection).
Factors in fistula healing
Early pus culture sensitivity testing and appropriate antibiotics.
Early percutaneous drainage and decompression of liver abscess.
Good nutritional status with high protein intake.
Good glycaemic control.
Early surgical intervention in patients not responding to minimally invasion surgery.
Learning points
Burkholderia is known to cause various visceral abscesses, including liver abscesses.
Burkholderia liver abscess rarely causes hepatobronchial fistula.
Purulent cough with a metallic taste in a patient with liver abscess should raise concern for hepatobronchial fistula.
Ethics statements
Patient consent for publication
Footnotes
Contributors NBP—planning, writing and submitting the case. HI, SC, IP—helped in writing the case.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.