Article Text

Statistics from Altmetric.com
Description
A 16-year-old female adolescent with a history of high-risk pre-B acute lymphoblastic leukaemia in remission after 2 years following chemotherapy and whole brain irradiation was seen for a follow-up oncological visit, where she was found to have suicidal indications. The patient’s mother had died 6 months previously due to pancreatic cancer. Following evaluation in the emergency room demonstrating absence of any focal neurological sign, she was transferred to an inpatient psychiatric facility. Five days following admission, she was sent to the emergency room for evaluation of altered mental status, atypical episodes of enuresis and headaches. Neurological exam revealed a depressed affect without neurological deficits. Head CT demonstrated a large, right frontal tumour with mass effect and significant obstructive hydrocephalus (figure 1A). MRI identified a large solid and cystic mass located within the right frontal and temporal lobes with reduced diffusivity and heterogeneous enhancement (figure 1B,C). The neuroradiographical differential diagnosis included high-grade glioma, anaplastic ependymoma or supratentorial embryonal tumour. History of radiation was most suggestive of a secondary malignancy. The patient underwent neurosurgical resection where histopathology revealed a hypercellular glial tumour with atypical nuclei, prominent mitoses and necrosis consistent with a diagnosis of high-grade glioma (figure 2). Next-generation sequencing on the tumour revealed a mutation in TP53 (Y126C) and variants of unknown significance in nine genes (ALK, ATRX, BRIP1, CIC, EP300, RB1, IRS2, PTCH1 and RANBP2). Germline testing revealed the same TP53 mutation. The patient received photon radiotherapy with concomitant temozolomide; unfortunately, she died 6 months after diagnosis from progressive disease.

Neuroimaging features of secondary high-grade glioma. (A) Head CT demonstrated a large, right frontal tumour with mass effect and significant obstructive hydrocephalus. MRI identified a large solid and cystic mass located within the right frontal and temporal lobes with reduced diffusivity (B) and heterogeneous enhancement (C).
{kind=link}
{kind=link}
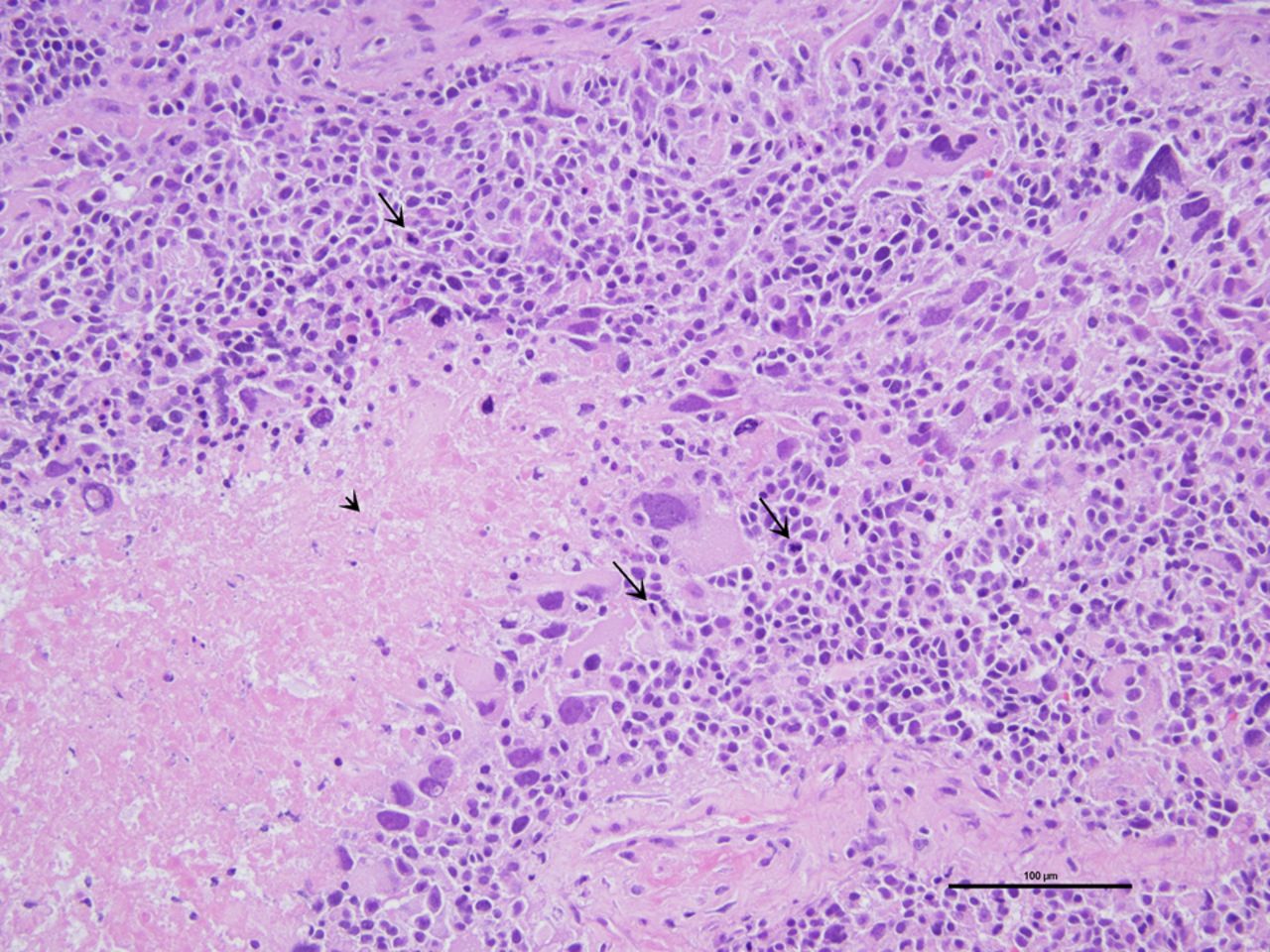
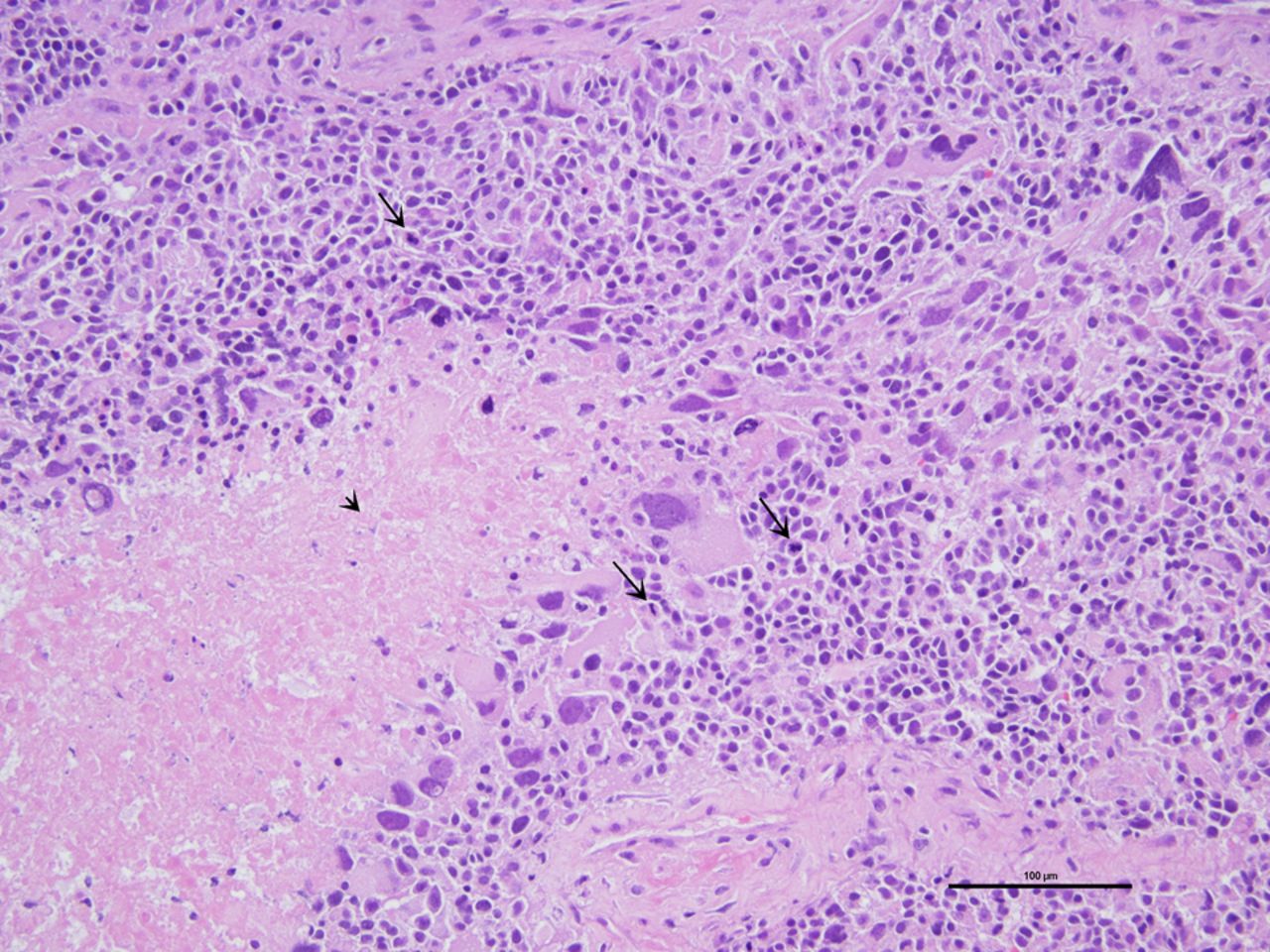
Neuropathology of secondary high-grade glioma. H&E-stained section reveals a malignant glial tumour with atypical nuclei, abundant mitoses (long arrows) and necrosis (arrowhead) consistent with a diagnosis of high-grade glioma.
Primary childhood brain tumours may uncommonly present with psychiatric symptoms such as psychosis, anxiety and changes in mood as opposed to more classical presenting features of headache and vomiting.1 Depression may be a rare psychiatric presenting symptom of high-grade glioma, with some cases presenting with normal neurological examination.2 The incidence of secondary malignancies presenting with primary psychiatric features is less understood. The overall cumulative incidence of brain tumours in children treated for childhood acute lymphoblastic leukaemia is under 2% based on a study population of 1612 consecutive patients treated at St. Jude Children’s Research Hospital.3 Only 10 of 1612 patients had developed high-grade glioma at a median latency of 9.1 years.3 Risk factors for secondary brain cancers include history of radiation therapy and germline mutations, both of which were present in our patient.3–5 Familial TP53 mutation, Li-Fraumeni syndrome, is a cancer predisposition condition which has been implicated in childhood acute lymphoblastic leukaemia with a risk of up to 50% within 49 years after first diagnosis of secondary malignancy.4 6
Our case highlights a primary psychiatric presentation of a secondary malignancy, even in the absence of any focal neurological signs. The absence of any neurological focal signs, given the size and neuroimaging characteristics, was unexpected. It is possible that rapid tumour growth and the anatomical location may have been contributing factors to explain the incongruence. The unique clinical presentation, together with the novel molecular features, adds to the diversity of secondary high-grade glioma of childhood.
Learning points
Psychiatric symptoms may be presenting features of childhood brain tumours, even in the setting of a normal neurological examination.
Patients with TP53 germline mutations (Li-Fraumeni syndrome (LFS)) are at higher risk of secondary malignancy following radiation therapy, with high consideration for secondary high-grade glioma.
Patients with LFS carry a high lifetime risk of cancer, non-specific to primary or secondary malignancies, and early germline testing in at-risk patients is suggested.
Ethics statements
Patient consent for publication
Footnotes
Contributors All authors were responsible for the design and writing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.