Article Text

Statistics from Altmetric.com
Description
A 61-year-old woman with a history of asthma presented to the emergency department with wheezing and dyspnoea. Her oxygen saturation was 82% while breathing ambient air, and a chest radiograph showed no signs of pneumonia or pneumothorax. Despite the use of epinephrine, bronchodilators and systemic corticosteroids, the patient’s respiratory condition did not improve and intubation was necessary on the day of the visit. Subsequently, pneumothorax developed on the right side and a chest tube was placed. On hospital day 3, crepitus appeared and spread from her head to her lower limbs. CT revealed right pneumothorax, pneumomediastinum and massive subcutaneous emphysema from the chest to the abdomen (figure 1). The patient’s subcutaneous emphysema with pneumothorax and the exacerbation of asthma gradually resolved, and she was extubated on hospital day 13.

{kind=link}
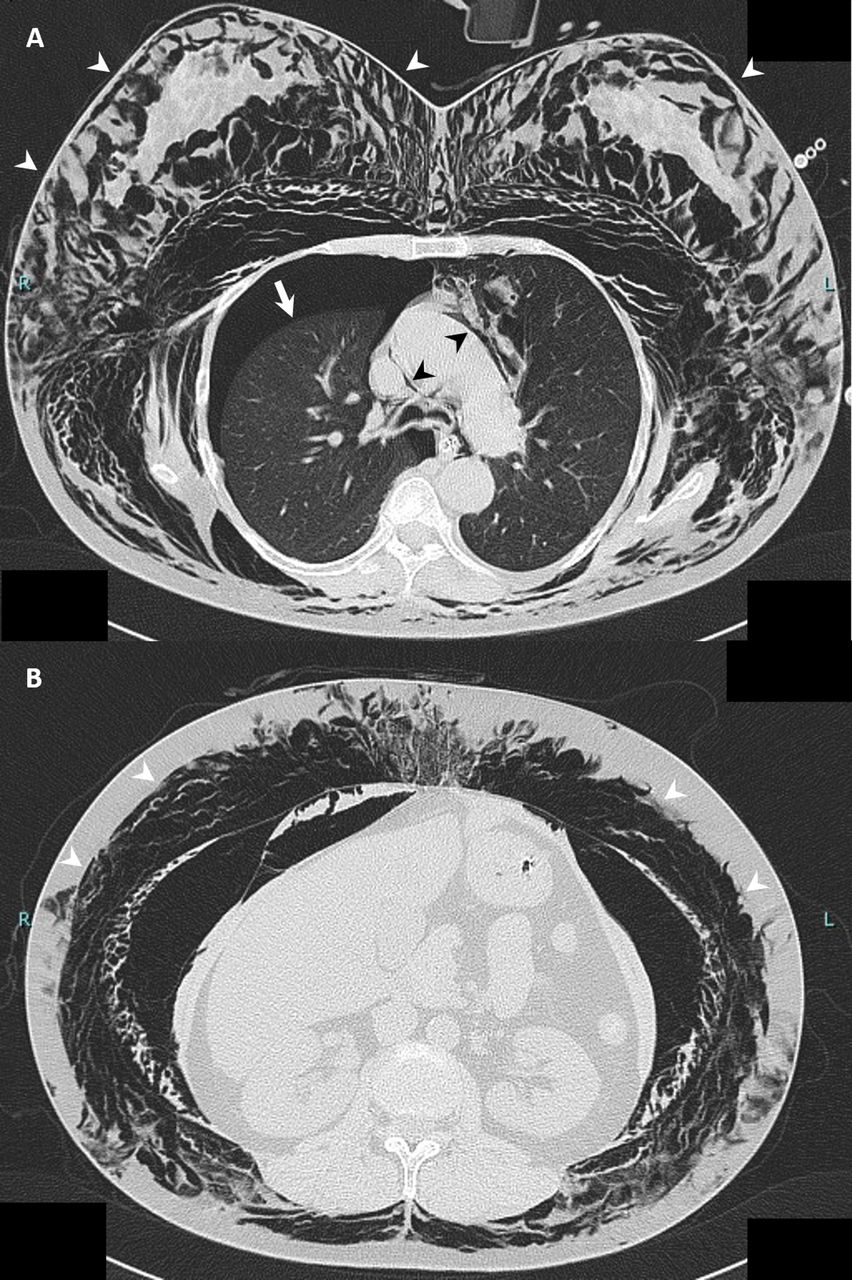
High-resolution CT showing right pneumothorax (A, arrow), pneumomediastinum (A, black arrowheads) and massive subcutaneous emphysema from the chest to the abdomen (A and B, white arrowheads).
A pathophysiological process of pneumomediastinum is known as the Macklin effect,1 which is summed up in three steps: alveolar ruptures, air dissection along bronchovascular sheaths and spreading of this pulmonary interstitial emphysema into the mediastinum. The Macklin effect is involved in pneumomediastinum that occurs in a variety of conditions, including asthma attack, blunt trauma, mechanical ventilation and Valsalva manoeuvres. As the mechanism of pneumomediastinum and subcutaneous emphysema in the present case, an increased intrathoracic pressure associated with asthma attack and mechanical ventilation might cause secondary alveolar hyperextension and rupture of the alveolar wall. The thoracic drainage for pneumothorax could also have an impact in the present case. The leaked air might travel through the sparse vascular sheath of the tissue and leak from the hilum to mediastinum, and an increased mediastinal pressure might form subcutaneous emphysema via the cervical fascia.1 Some increased mediastinal pressure might enter the right pleural space after a rupture of mediastinal pleura.
Patient’s perspective
I will be glad to be of help for the future healthcare.
Learning points
An increased intrathoracic pressure associated with asthma attack and mechanical ventilation due to the Macklin effect may form mediastinal emphysema. If it progresses further, it may cause subcutaneous emphysema and pneumothorax.
The thoracic drainage for pneumothorax may enhance subcutaneous emphysema.
Ethics statements
Patient consent for publication
Footnotes
Contributors TI and HI researched the topic and wrote the case. YK and HK helped with the research and proofreading of the case report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.