Article Text

Statistics from Altmetric.com
Description
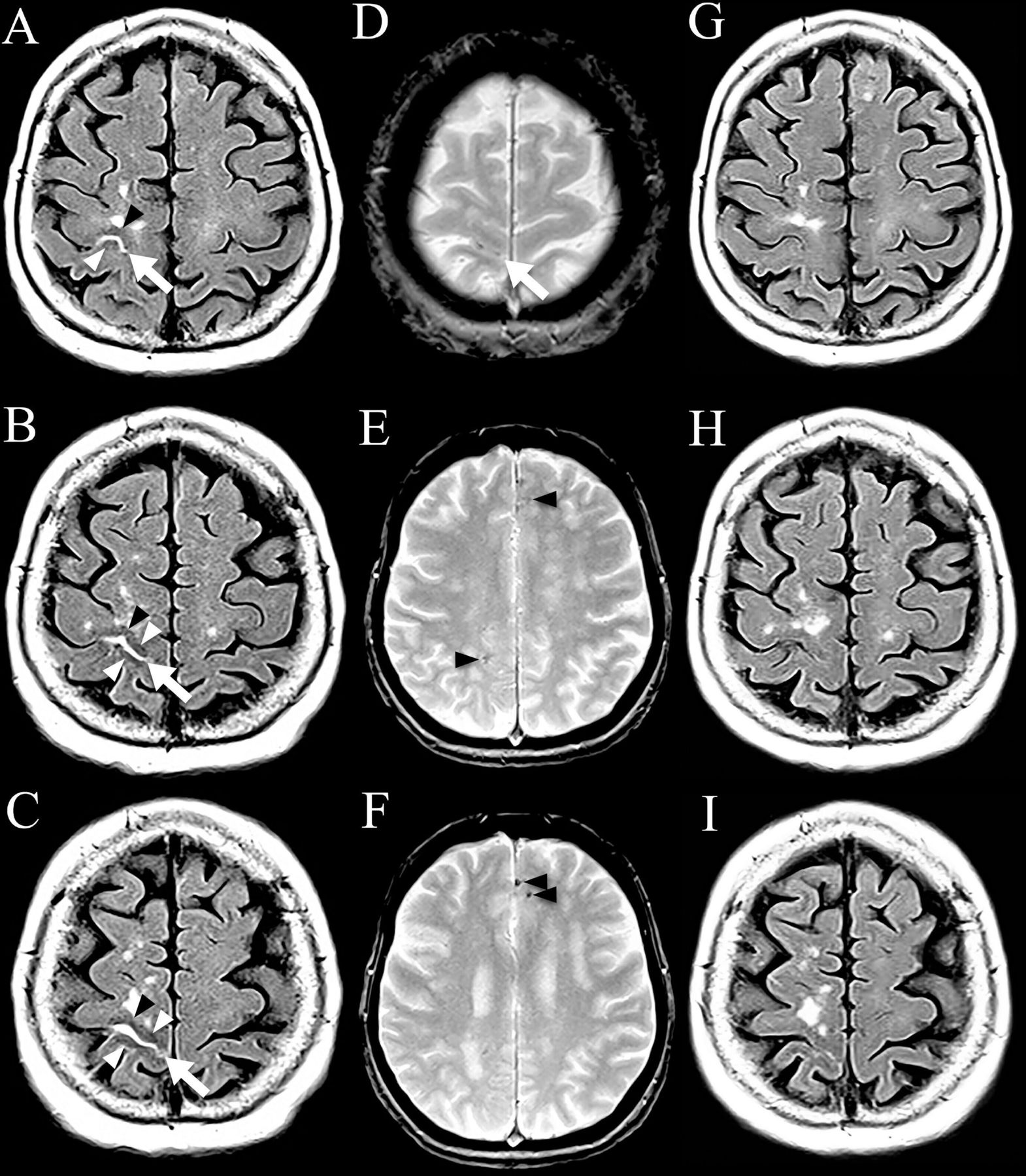
A 69-year-old woman presented with transient spreading sensory symptoms in the left upper limb compatible with a transient focal neurological episode (TFNE). MRI performed 3.5 hours later revealed an acute focal right rolandic convexity subarachnoid hemorrhage (cSAH), seen as hyperintensity on fluid-attenuated inversion recovery (FLAIR; figure 1A–C, arrows) and as hypointensity on T2*-weighted imaging (figure 1D, arrow). Associated FLAIR hypointensities were observed in the corticosubcortical brain areas adjacent to the cSAH (figure 1A–C, arrowheads), with a mean signal intensity of 139 in the visually involved right perirolandic corticosubcortical area compared with a mean signal intensity of 174 in the contralateral left perirolandic corticosubcortical mirror area. Diffusion-weighted imaging (and apparent diffusion coefficient) were strictly normal. Multifocal cortical superficial siderosis on T2*-weighted imaging (figure 1E,F, arrowheads) evoked underlying cerebral amyloid angiopathy (radiological abnormalities corresponded to possible cerebral amyloid angiopathy according to the modified Boston criteria). Two weeks later, the subarachnoid and adjacent corticosubcortical FLAIR signal changes normalised (figure 1G–I), with a mean signal intensity of the corresponding earlier involved perirolandic corticosubcortical area of 172 on the right and 173 on the left side.

{kind=link}
MRI showing right rolandic cSAH seen as FLAIR hyperintensity (arrows) associated with hypointensity (arrowheads) in the adjacent cortex (A–C). T2*-weighted imaging showed cSAH (D, arrow) and associated multifocal cortical superficial siderosis (E and F, arrowheads) evoking underlying cerebral amyloid angiopathy. Two weeks later, FLAIR signal changes normalised (G–I). cSAH, convexity subarachnoid hemorrhage; FLAIR, fluid-attenuated inversion recovery.
Transient subcortical FLAIR hypointensity has been described in different disorders, including seizures (often associated with non-ketonic hyperglycaemia), ischaemia, multiple sclerosis, leptomeningeal metastasis, meningitis/meningoencephalitis, Sturge-Weber syndrome, moyamoya disease.1–3 The decreased subcortical signal intensity on FLAIR is thought to be related to non-haem iron (a feature of early ischaemia) accumulation and presence of free paramagnetic (because of their unpaired electrons) radicals possibly related with excitotoxic damage.
The exact underlying pathophysiology of TFNE is unknown. The typically spreading nature of symptom onset, the short duration and the stereotyped character of symptoms suggest focal seizure activity, cortical spreading depression or local vasospasm, related to the presence of fresh blood or blood-breakdown products accumulating in superficial cortical layers of the involved sulci.4 Transient corticosubcortical signal changes (never earlier reported to the best of our knowledge) as observed in our patient presenting with acute focal cSAH and TFNE may help to better understand the underlying pathophysiology of symptoms in TFNE.
Learning points
Transient subcortical fluid-attenuated inversion recovery hypointensity, thought to be related to non-haem iron (a feature of early ischaemia) accumulation and presence of free paramagnetic (because of their unpaired electrons) radicals possibly related with excitotoxic damage, can be observed in different brain disorders.
Transient corticosubcortical signal changes (never earlier reported to the best of our knowledge) as observed in our patient presenting with acute focal convexity subarachnoid hemorrhage and transient focal neurological episode (TFNE) may help to better understand the underlying pathophysiology of symptoms in TFNE.
Ethics statements
Patient consent for publication
Footnotes
Contributors DR contributed to planning, conduct, reporting, conception and design, acquisition of data or analysis and interpretation of data. EEH contributed to planning, conduct, reporting, conception and design, acquisition of data or analysis and interpretation of data. MP contributed to planning, conduct, reporting, conception and design, acquisition of data or analysis and interpretation of data. ET contributed to planning, conduct, reporting, conception and design, acquisition of data or analysis and interpretation of data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.