Article Text

Abstract
A 28-year-old male was referred by his local general practitioner due to recurrence of painful right scrotal mass, first noted 8 years prior. The mass was further characterised with ultrasound and then was locally excised via an inguinal approach, sparing the testicle, without any postoperative complication. Immunoperoxidase staining of the excised lesion confirmed paratesticular IgG4-related disease.
- rheumatology
- surgery
- urological surgery
- ultrasonography
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
IgG4-related disease (IgG4-RD) is an immune-mediated fibroinflammatory condition that may affect multiple organs. Paratesticular involvement in IgG4-RD is relatively uncommon, and when it occurs, it usually presents as benign paratesticular lesions.1 2 A better understanding of the diagnostic process associated with benign paratesticular mass is crucial to aid treatment decision-making and avoid unnecessary invasive management, such as radical orchidectomies.
We report a case that highlights the workup, management and outcome of a benign paratesticular fibrous pseudotumour (PFP) secondary to IgG4-RD with a testicular-sparing surgical excision.
Case presentation
A 28-year-old man presented with a right scrotal mass associated with intermittent throbbing scrotal pain that was amendable to non-steroidal anti-inflammatories. There were no associated infective or constitutional symptoms. The patient was a sexually active, heterosexual male with single long-term partner. He has no other comorbidities with no history of trauma, surgery or infection.
Similar symptoms were reported 8 years prior and were associated with sonographic evidence of moderately enlarged right epididymis. He was empirically managed for suspected epididymitis with oral course of antibiotics prescribed by his local general practitioner with no subsequent follow-up.
Clinical examination revealed a mildly tender, firm palpable mass above, and likely not involving, the right testicle.
Differential diagnosis
Most of the epididymal lesions are attributed to benign cases, with adenomatoid tumour of the epididymis being the most common. Other differential diagnoses can include benign epididymal cysts, sarcoidosis and infective aetiologies, such as tuberculosis and epididymal abscess. Malignant epididymal lesions are relatively rare and can be due to primary tumour, such as epididymal leiomyosarcoma or metastases. Certain clinical attributes, such as more acute pain presentation and associated systemic symptoms, can differentiate some infective pathologies compared with other causes. The presence of colour Doppler flow can also be beneficial in distinguishing malignant from benign lesions.3 4
Investigations
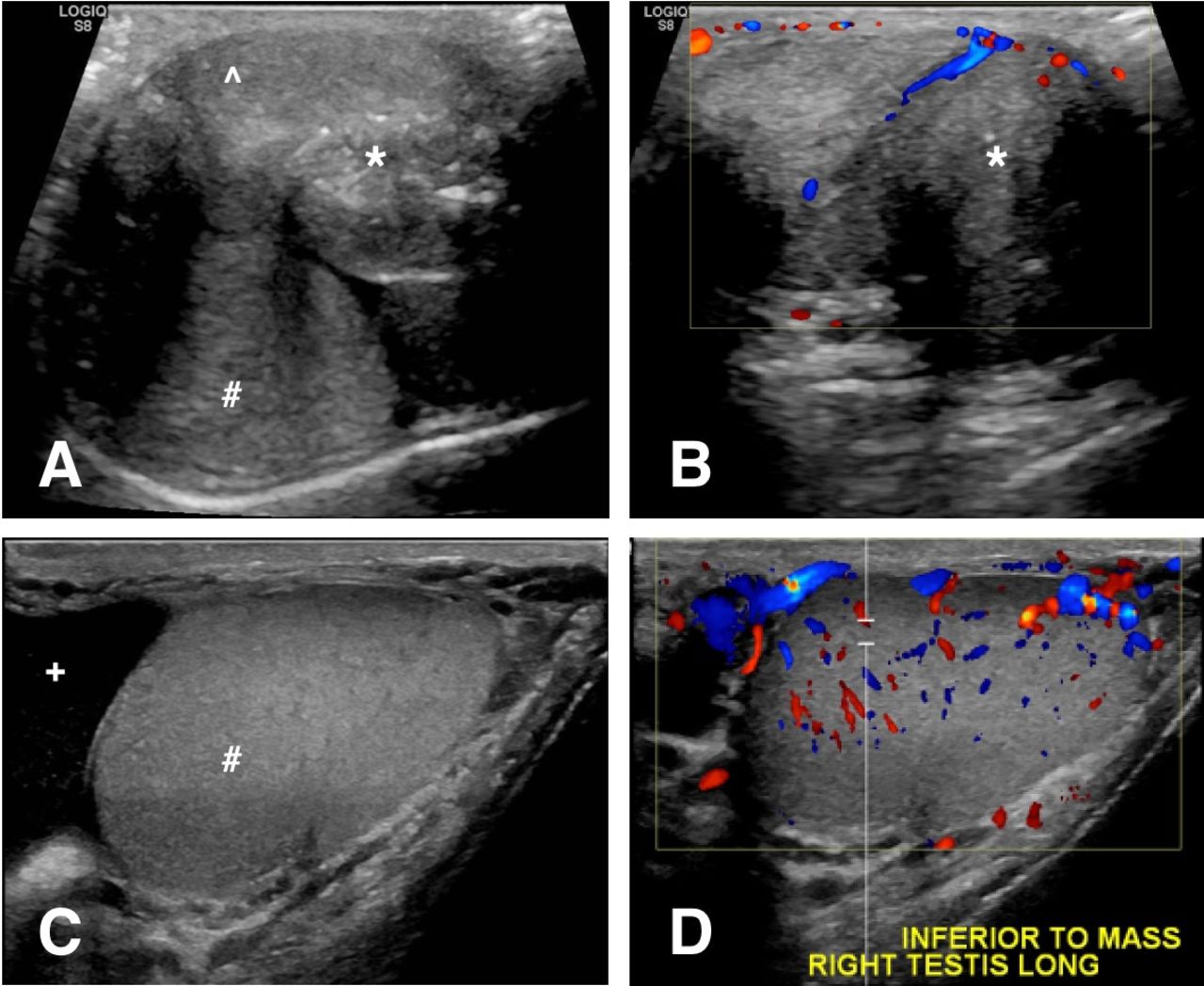
Atypical infection screen was performed considering the patient’s duration of symptoms, including for schistosomiasis and tuberculosis, with negative results. Scrotal ultrasound (US) showed a grossly enlarged and heterogeneous right epididymal mass with coarse calcifications and shadowing measuring approximately 91×62×41 mm, causing inferior displacement of the ipsilateral testis (figure 1). The other finding included a single right 20 mL hydrocele. Both of his testes were of normal size, echotexture and vascularity.

(A) Transverse sonographic view of right scrotal mass likely arising from the epididymis (∧) with coarse calcifications (*) causing displacement of the right testicle (#). (B) Transverse sonographic view of the heterogeneous and relatively avascular scrotal mass (*). (C) Longitudinal view of the normal-appearing right testicular tissue in its displaced position with adjacent right hydrocele (+). (D) Longitudinal view of the normal right testicular tissue inferior to the mass with normal vascularity on colour Doppler imaging.
Treatment
The patient underwent a right scrotal exploration and testicular-sparing epididymectomy via an inguinal approach. Intraoperative findings included a large multinodular solid mass arising from the epididymal tail (figure 2). The testis was normal and uninvolved. The epididymal tail and mass were dissected off the testis, and the epididymal artery was selectively ligated, with preservation of the testicular vascular supply. He tolerated the procedure and was discharged on the same day.

Intraoperative images of (A) the multinodular paratesticular lesions (*) with normal-appearing right testicle (#) prior to excision and (B) the site following the testicular-sparing excisions, with the right testicle in view (#).
Outcome and follow-up
Histology from the excised specimen showed dense fibrotic stroma with scattered spindle cells and numerous infiltrative plasma cells and lymphocytes. The presence of plasma cells was further confirmed with several immunoperoxidase stains, including for IgG. Positive staining with IgG4 in some areas were up to 50% of the IgG cells, confirming the diagnosis of IgG4-related benign fibrous pseudotumour (figure 3). There was no evidence of any necrosis or granulomas. The histopathology result was communicated to the patient on his clinic follow-up. There was no recurrence 6 months following his surgery.

{kind=link}
{kind=link}
{kind=link}
(A) Histopathology sections of right epididymal mass with H&E stain showing storiform fibrosis and lymphoplasmocytic infiltrate (×200), as well as (B) plasma cells (×200). Further immunohistochemistry confirms the presence of (C) IgG-staining cells (×200) and (D) IgG4-staining plasma cells (×200).
Discussion
PFP is a benign reactive fibrous lesion that may arise from tunica vaginalis, tunica albuginea or the epididymis.1 5 6 PFP is uncommon and represents around 6% of paratesticular tumours.2 They typically present with palpable, mobile, multinodular, painless scrotal mass.3 Microscopically, the nodules usually comprise dense fibrous tissue and fibroblasts with the presence of inflammatory cells and varying degrees of calcifications.7 Miyamoto et al categorised PFP into three subtypes, namely, those with myofibroblastic changes, those with inflammatory sclerotic changes and those with plaque-like appearance without significant inflammation.1 Although the pathophysiology remains unclear, it was thought that PFP might be clinically correlated with a history of hydrocele, trauma or infection. This was demonstrated by Mostofi et al, which identified 30% and 45% of PFP cases to be associated with trauma and hydrocele, respectively.8 Similarly, Miyamoto et al showed 46% of their cases have prior or concurrent evidence of hydrocele.1
Bösmüller et al introduced the idea of reclassifying PFP as a localised manifestation of IgG4-RD based on the abundance of IgG4-positive plasma cells and elevated IgG4/IgG ratio of 44%–48%.5 This was further supported by Hart et al, who reported a case of PFP 6 years following completion of long-term corticosteroids for autoimmune pancreatitis and retroperitoneal fibrosis with elevated serum IgG4.9 Similar to PFP, IgG4-RD is a rare disorder with varying organ involvements, which now include sclerosing autoimmune pancreatitis, sclerosing cholangitis, retroperitoneal fibrosis, Riedel’s thyroiditis, interstitial pneumonitis and others.1 5 7 9 The incidence of IgG4-RD was estimated to be around 0.28–1.08 per 100 000 people. Those affected are more commonly middle-aged to elderly men with a median age at time of diagnosis of 58.8 years. Less than 10% of cases were diagnosed before 40 years of age.10 11 Patients typically present subacutely, some with relapsing-remitting course or long plateau.12–14 Uchida et al proposed the diagnostic criteria for definite IgG4-RD to include (1) the presence of mass, nodule, organ enlargement and/or dysfunction; (2) elevated serum IgG4 concentration >135 mg/dL; and (3) the presence of >10 IgG4 cells in high-power field and an IgG4/IgG cell ratio of >40%.15
Three histological features are commonly present in IgG4-RD, which include storiform fibrosis, obliterative phlebitis and lymphoplasmacytic infiltrate. Storiform fibrosis is considerably the hallmark feature of IgG4-RD and is typically characterised by radially arranged collagen fibres that may represent a cartwheel spoke. Obliterative phlebitis is the complete or partial obstruction of small and medium-sized veins, which may be attributed to lymphoplasmacytic infiltrate or external compression. Lymphocytic infiltrate commonly includes B cells organised in germinal centres and widespread T cells, in particular CD4-positive T cells. The diagnosis of IgG4-RD usually involves the presence of IgG4-bearing plasma cells. Eosinophils may also be identified but is not required in the diagnosis. Several other features, such as neutrophils, necrosis, increased mitotic activities and granulomas, are uncommon and may point towards alternate diagnoses but can be present in certain site-specific IgG4-RD.12–14 16
Compared with IgG4-RD in general, paratesticular manifestation of IgG4-RD more commonly affects younger men with a median age of 30 years (range, 19–74 years).5 9 17–22 The subacute presentation of painless scrotal mass in young men commonly prompted clinicians to consider radical orchidectomy due to suspicion of malignancy. US, despite frequently used, may not be sufficient to form such diagnosis. Under US, PFPs may present either as hypoechoic or as hyperechoic lesions depending on the levels of calcifications and collagenous tissues.23 In several cases, US is sufficient to isolate lesions arising from the spermatic cord and tunica vaginalis, which have led to testicular-sparing excisions.18 21 24 The findings, however, will still need to be corroborated with intraoperative findings as highlighted by Shams et al, which identified necrotic testicular tissue despite reportedly normal testicle on prior US.25 Other features that may be present include small to moderate amount of vascularity and the presence of ipsilateral hydrocele.22–24
In terms of serology, elevated serum IgG4 concentrations may also not be sufficient to confirm the diagnosis of IgG4-RD. In their review article, Kamisawa et al highlighted that IgG4-RD can still be diagnosed in the setting of normal serum IgG4, with 20% with type 1 autoimmune pancreatitis being shown to have normal level on presentation.13 Serum IgG4 level can also be elevated in other diseases, such as atopic dermatitis, asthma, pemphigoid, multicentric Castleman disease and some malignancies.13 15 Serum IgG4 level may be of benefit for monitoring disease progression and/or response to therapy. Kim et al reported higher concentration on presentation with paratesticular and retroperitoneal involvement.20 The level has also been shown to decline following commencement of glucocorticoids, likely signalling good response.13 In a case of paratesticular IgG4-RD without no other organ involvement published by Mochizuki et al, they found that serum IgG4 was normal following orchidectomy.22 Although this might be difficult to assess considering the absence of serology result prior to surgery, it may indicate the potential use of serum IgG4 to prognosticate single organ manifestation of IgG4-RD following surgical intervention.
Preoperative imaging and/or biopsy are often the deciding factor for choice and extent of surgical intervention, which tend to be associated with the risk of malignancy and questions surrounding the viability of testis. Similar to the aforementioned investigations, preoperative biopsy may not necessarily answer the two questions. Mochizuki et al performed a scrotopuncture, which showed some plasmacytes and small, unvarying lymphocytes, features that did not improve clinical confidence for exclusion of malignancy.22 Clinicians may also consider the adoption of intraoperative frozen section analysis as it is thought to confirm the benignity of the lesions and hence avoid unnecessary orchidectomy.21 Gordetsky et al evaluated the use of frozen section in five PFP cases. Of the five cases, four were considered benign, but two proceeded to have orchidectomy following concerns of testicular involvement instead of testicular-sparing local excisions. From the latter two cases, one showed testicular atrophy with diffuse chronic inflammations, while the other was unremarkable. The frozen section of the last case subjected to orchidectomy revealed dense fibrocollagenous tissue with lymphoid aggregates, leading to difficulties in excluding lymphoproliferative disorders.26 Regarding the surgery, no complications were reported in prior cases with patients having good outcome, some recurrence-free of up to 12 years.17 18 Nevertheless, in the event of recurrence, clinicians need to be mindful of possible recurrence in contralateral or distant sites.
Learning points
Paratesticular IgG4-related disease (IgG4-RD) should be considered as one of the differential diagnoses for subacute presentation of scrotal mass as its benign nature can involve medical management or less invasive surgical approach
Paratesticular involvement in IgG4-RD is less common when compared with other organs, but possible as an initial presentation or recurrence of the disease
Testicular-sparing surgical excision of IgG4-related paratesticular lesions provides comparable recurrence-free outcomes when compared with radical orchidectomy
Ethics statements
Patient consent for publication
Acknowledgments
Histological images provided by Dr Philip Kostos, MBBS, FRCPA, Medical Director, Anatomical Pathology, Dorevitch Pathology, Footscray Hospital, Victoria, Australia.
References
Footnotes
Contributors NAS was involved in case curation, writing the original draft, and review and editing. JK was involved in conceptualisation, case curation, review and editing. IP was involved in review and editing. DK was involved in conceptualization, review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.