Article Text

Abstract
Myocardial infarction with non-obstructive coronary arteries (MINOCA) is a rare form of acute myocardial infarction and it is an even rarer cause of ventricular septal defect (VSD). We present a case of successful endovascular closure of post-MINOCA VSD with the use of an atrial septal defect (ASD) occluder. The patient improved from intra-aortic balloon pump dependent to New York Heart Association (NYHA) I in a matter of days. 18-month follow-up period is event free and symptom free.
- cardiovascular medicine
- interventional cardiology
- interventional cardiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Ventricular septal defect (VSD) caused by myocardial infarction with non-obstructive coronary arteries (MINOCA) is an extremely rare entity. There is no standard protocol or guideline for action. Numerous advancements in devices and techniques in the field of endovascular medicine have made it a possible alternative to surgery for the treatment for this rare condition. We present, to the best of our knowledge, the first report of endovascular closure of MINOCA-caused VSD.
Case presentation
A 78-year old woman presented to our clinic late (48 hours) after chest pain onset, dyspnoea, heart failure NYHA III and rapidly deteriorating haemodynamic. The patient’s blood pressure was 100/65 mm Hg, heart rate—130 beats/min, respiratory rate was 20 breaths/min and oxygen saturation was 94% on room air. Physical examination was notable for a grade III/IV systolic murmur at the apex of the heart, propagating towards the left sternal border.
The patient had a history of hypertension stage III, paroxysmal atrial fibrillation and diabetes type II. She had survived an ischaemic stroke 10 years ago, total hysterectomy 15 years ago and right kidney resection 17 years ago.
Investigations
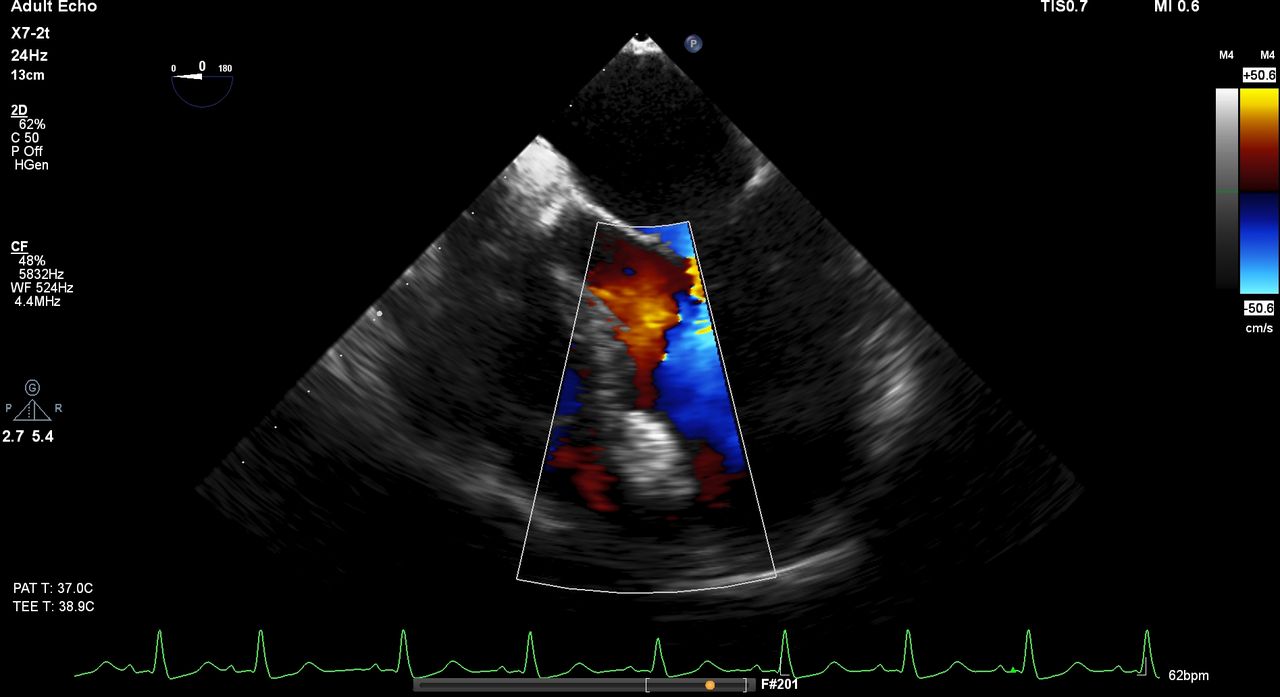
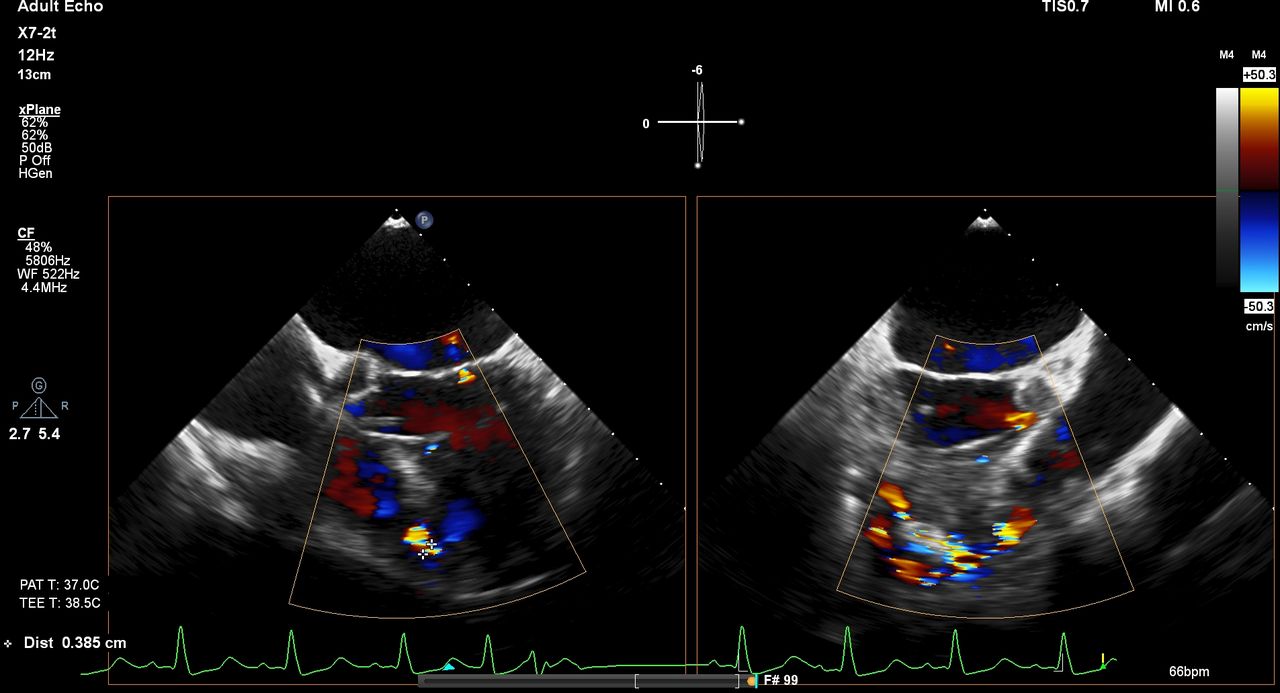
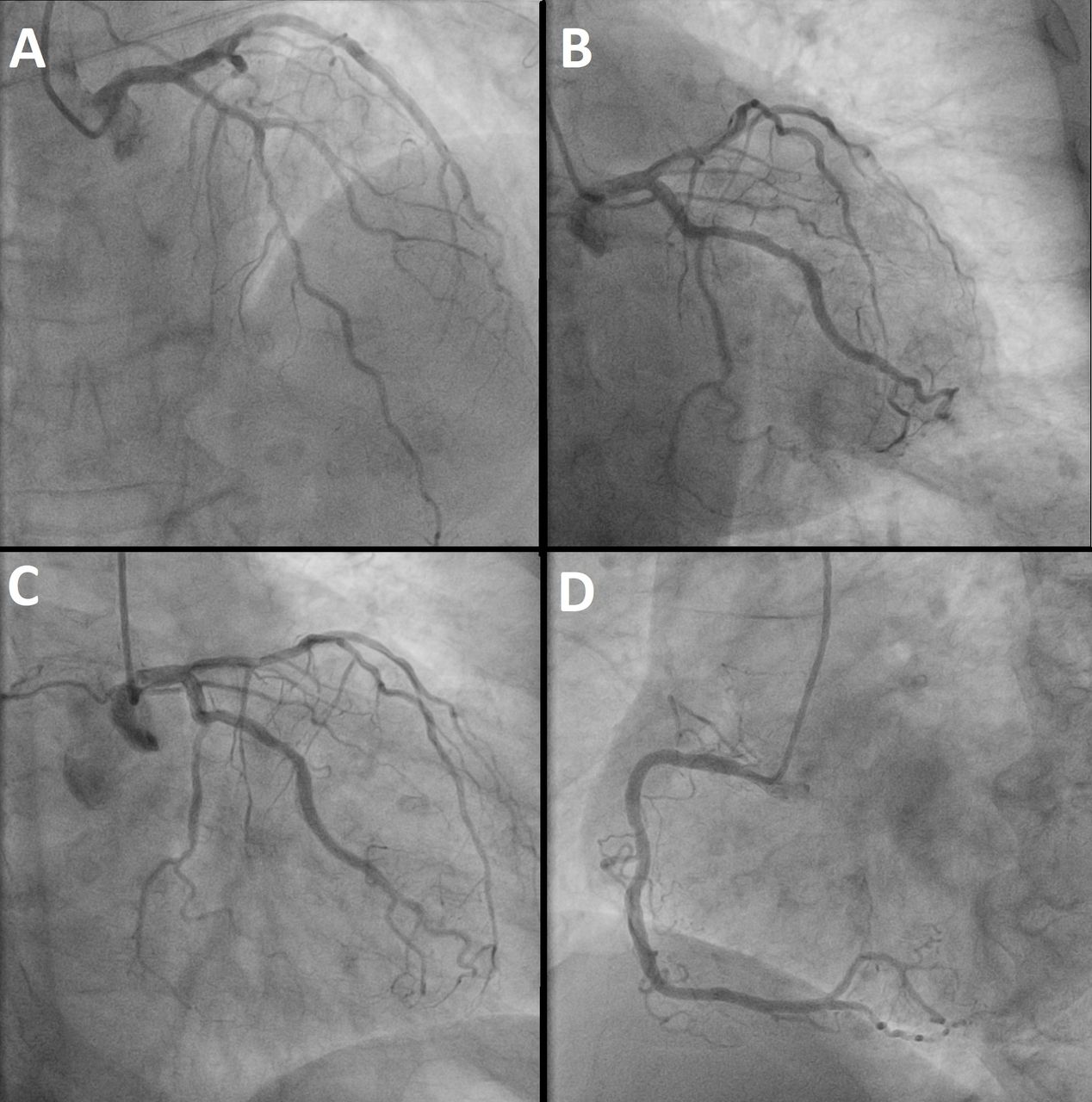
On ECG, the patient had a new left bundle branch block with secondary repolarisation changes in all leads (figure 1). Laboratory results were remarkable for creatine kinase (CK) of 246 U/L, CK-MB—48 U/L, troponin I hs—478 ng/L. Transthoracic echocardiography (TTE) showed left ventricle ejection fraction (LVEF) of 40%, with septo-apical hypokinesia, IInd degree mitral regurgitation, tricuspid regurgitation grade III and elevated right ventricle systolic pressure of 63 mm Hg. VSD in the low-mid septum was visualised with a size of 7/12 mm. Immediate coronary angiography showed no atherosclerotic obstructive disease, neither dissection, nor coronary spasm (figure 2). Transesophageal echocardiography (TEE) and 3D-Echo were performed (figures 3–4, videos 1 and 2). CT a few days later sized the muscular defect as 0.9 cm wide with height and width of the defect orifice on the side of the left ventricle of 0.83 cm and 2.0 cm, respectively (figure 5). The findings were consistent with VSD caused by MINOCA. In the context of paroxismal atrial fibrillation, we assumed that the MINOCA in our case was caused by coronary embolism. VSD is a rare complication of acute myocardial infarction (AMI) and an even rarer complication of MINOCA (only 10 cases reported to date).

ECG on presentation. ST-elevations in V1–V5 can be seen in addition to new left bundle branch block, both diagnostic for a myocardial infarction.

Emergent angiography. (A–C) No significant stenosis or occlusions are evident in the left coronary artery system. (D) Right coronary artery is clear or significant stenosis or occlusions.

Transesophageal echocardiography (TEE) before the procedure. Echocardiography measured the muscular part of the defect as 7 mm wide at its narrowest point.

Three-dimensional (3D)-echocardiography before the procedure. The defect was visualised and assessed on 3D echo.

CT scan before the procedure. (A) Size of the ventricular septal defect orifice on the side of the left ventricle. (B) Size of the muscular part of the defect.
Differential diagnosis
The differential diagnosis between MINOCA and obstructive AMI can be made only by coronary angiography. Distinguishing acute mitral regurgitation from ventricular septal rupture after AMI is difficult based only on the murmur heard, and the colour flow Doppler echocardiography comes as method of choice.
Treatment
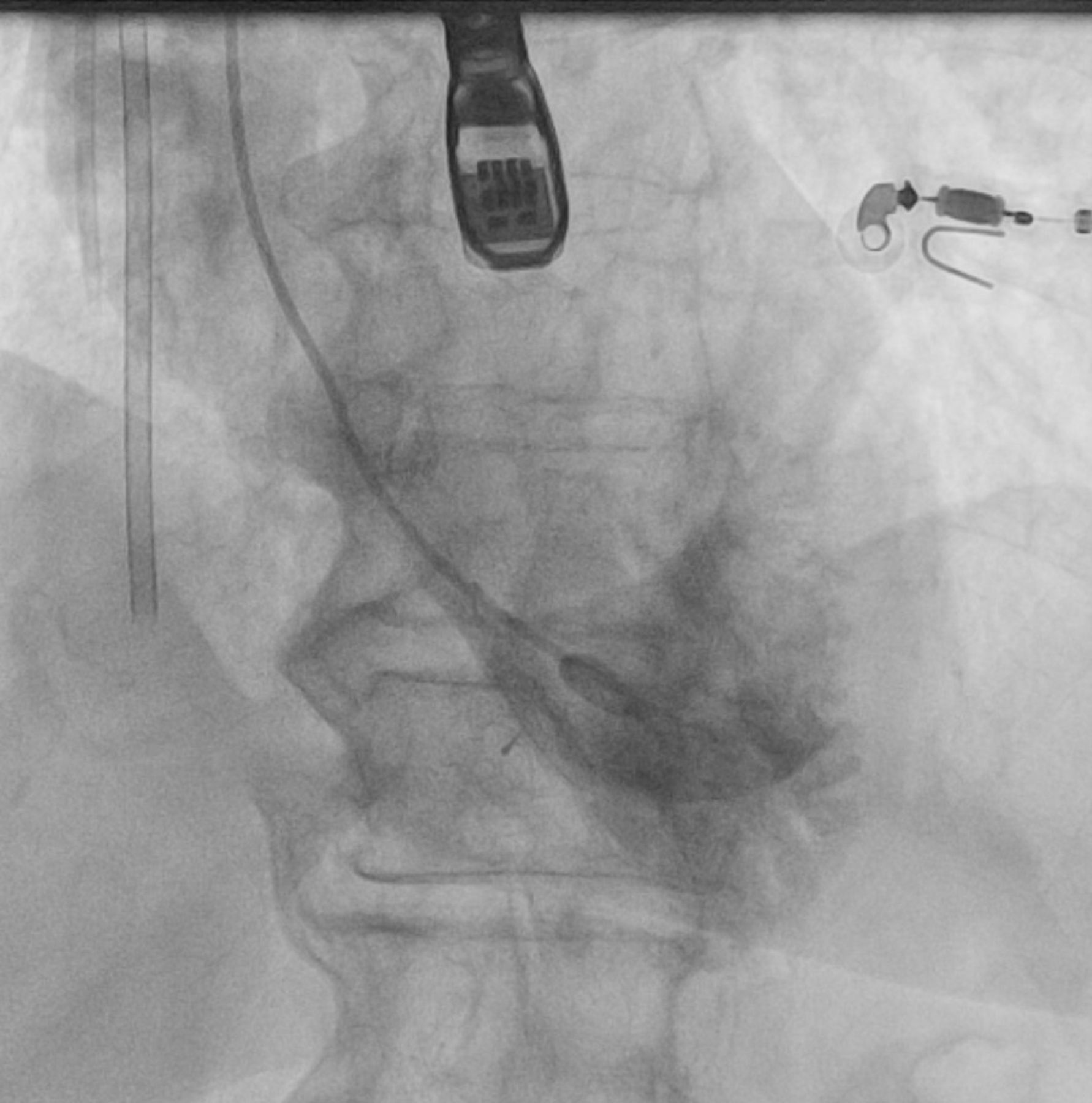
Due to the rapidly deteriorating haemodynamics, the patient was transferred to the intensive care unit and an intra-aortic balloon pump (IABP) was placed. Twenty-five days after the initial admission, a percutaneous VSD closure was performed. TEE was used in addition to fluoroscopy during the procedure. Through right radial artery, a left ventriculography was performed in LAO 50/CRA 30 revealing a close to normal global LV systolic function and a large VSD in the low mid muscular portion of the septum with significant left to right shunt (QP/QS measurements of 1.8/1.0) (figure 6, video 3). Using a 4 Fr Multipurpose GlideCath catheter (Terumo, Japan) and a 0.035″, Angled Radifocus Guide Wire M (Terumo, Japan) the defect was crossed and they were placed in superior vena cava. The wire was snared with a 25 mm Amplatz Goose Neck snare (Medtronic, USA) and externalised by the right jugular vein access followed by the GlideCath, providing a secure and stable arteriovenous loop (video 4). The wire was exchanged for a 260 cm 0.035″ STORQ wire (Cordis, UK). Using this through-and-through access, a 7F delivery sheath was introduced through the right jugular vein and positioned in the left ventricle across the VSD a Flex II atrial septal defect (ASD) occluder 29ASD09 (Occlutech, Germany) was introduced. Under both fluoroscopic and TEE guidance, the occluder was advanced across the VSD and intro the left ventricle. After secure positioning, the device was released (figures 7–8,videos 5–8). Final angiography showed immediate almost complete isolation of the VSD (figure 9, video 9).

Left ventriculography before device implantation. Massive shunt between the left and right ventricle is visualised.
Transesophageal echocardiography (TEE) during the procedure. Stable positioning of the atrial septal defect occluder device.
Transesophageal echocardiography (TEE) during the procedure. Drastic reduction of the shunt.

Left ventriculography after device implantation. Almost complete isolation of the shunt is visualised.
Outcome and follow-up
The patient was wined off the IABP on the next day and discharged 7 days later with significantly improved LVEF and clinical condition. She was reclassified from NYHA III to NYHA I. At 18-months follow-up, TTE showed that the device was firmly positioned and the shunt was completely sealed, the LVEF had increased to 62% and the systolic pressure in RV had decreased to 29 mm Hg (figure 10, video 10). The patient had neither problems nor clinical events.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
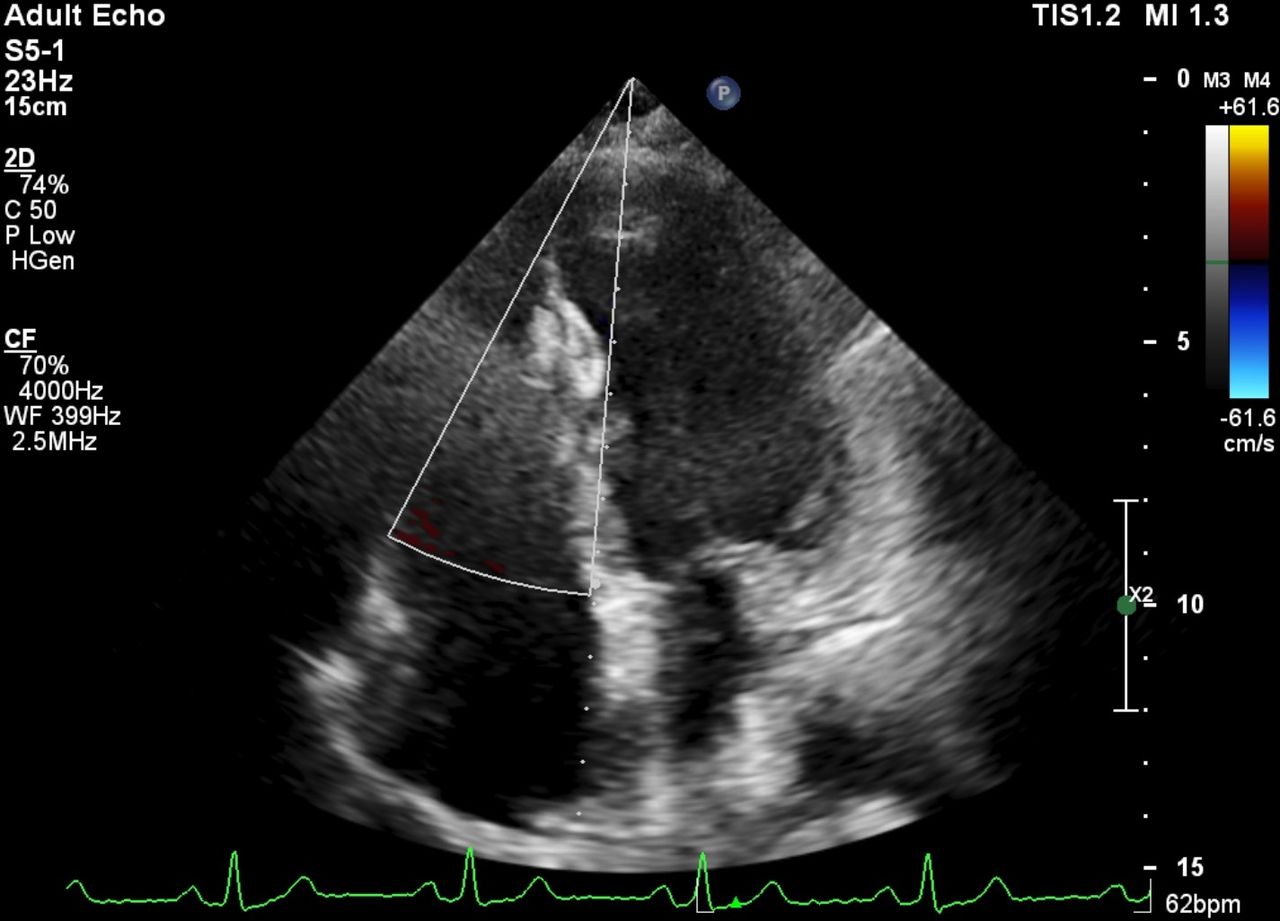
Echocardiography 18 months after the procedure. Atrial septal defect occluder device is firmly positioned in place and no shunt is visualised.
Discussion
A study involving 41 021 patients with myocardial infarction (MI) found that VSD occurred in 0.2% of the cases in the pre-percutaneous coronary intervention (PCI) era. Mortality at 30 days among those patients was more than 10 times higher than in those without this complication. Patients with VSDs in GUSTO-I (Global Utilization of t-PA and Streptokinase for Occluded Coronary Arteries) selected for surgical repair had better outcomes than those treated medically.1
Natural history data suggest a 2-month mortality rate of 90% after diagnosis in patients who do not undergo closure of the VSD.2 The poor survival rate forced us to make a plan for action. After the Heart team discussion, the patient was deemed too high-risk for open-heart surgery at this moment and the only other available option was endovascular closure of the VSD, awaiting further stabilisation and surgery or conservative treatment. The classical treatment is coronary artery bypass grafting (CABG) plus VSD closure, in our case the CABG was unnecessary and the less invasive endovascular treatment seemed like an appropriate alternative.
MINOCA accounts for average 6% of all AMI cases3 and the occurrence of complications with MINOCA is considered lower than in ‘standard’ infarction. After meticulous research, we found only 10 published cases of MINOCA-caused VSDs.4–13 All of them treated surgically with an overall survival rate of 60%. We did not find a case of post-MINOCA VSD treated by percutaneous approach.
Several studies described percutaneous closure of VSD after AMI as an alternative to surgery.14–16 The two largest studies investigating post-AMI VSD closed by percutaneous approach are by Asenza et al and Calvert et al. They include 40 and 53 patients, respectively.14 15 The patients in the first study had a 77% survival rate 30-days post VSD closure.14 In the second study, 58% of the patients survived to discharge. Average mid-term follow-up of patients after hospital discharge was for 395 days (first and third quartiles, 63–1522) days, during this time, only 4 patients died.15
The study by Thiele et al included 29 patients with post-AMI VSD immediately treated by percutaneous device closure. Their overall 30-day survival rate was 35%. They showed that successful closure of the defect is not the only factor defining survival. Time to intervention, cardiogenic shock, inotropic support, haemodynamic stability, age and comorbidities were also crucial.16
Those studies gave us proof that closure of the VSD is technically feasible and could be accomplished with a relatively low risk of major periprocedural complications. The question was when to perform the procedure. Data showed mortality rate after postinfarction VSD closure surgery is as high as 50% with lower rate when surgery is delayed.17
A retrospective study performed among 41 patients with post-AMI VSD found that the most important factor determining operative mortality and intrahospital survival is the time from the onset of AMI to surgery. Serpytis et al reported a 100% survival rate in patients surgically treated after 3–4 weeks of stabilisation versus 100% mortality in patients having surgery within 10 days from symptoms onset.18
We decided that delaying the VSD closure until haemodynamic stabilisation and further planning of the procedure would increase our chance of success and patient’s chance of survival. This additional time before the device implantation allowed stabilisation of the edges of the defect and scarring of the tissue surrounding the VSD to occur, providing firmer support of the closure device.
CT imaging was used for sizing of the device. We decided that ASD occluder is the best suit for our case because it provides a narrow shaft between the disks, ensuring avoidance of additional tissue damage during the delivery and a big enough disk area to ensure sealing of the defect even in the case of a subsequent enlargement. We considered the device best fitting to our case was Occlutech Flex II ASD occluder 29ASD09 (left atria disc size of 20.5 mm/ right atria disc of 16.5 mm and device waist of 9 mm).
Patient’s perspective
After the procedure my condition improved dramatically. A month after I was discharged from the hospital I was fully back to my normal life. I consider the procedure life-saving. I will be thankfulto the doctor to the end of my life.
Learning points
The echocardiographic and CT imaging is crucial for the ventricular septal defect (VSD) diagnosis and treatment.
The post-myocardial infarction with non-obstructive coronary arteries (MINOCA) VSD is a rare but potently fatal complication that requires timely diagnosis and efficient treatment.
Endovascular closure of post-MINOCA VSD could be an alternative to surgical treatment.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors ISP and ZIS: planning, conduct, conception and design. DBB and MS: reporting, acquisition and interpretation of data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.