Article Text

Statistics from Altmetric.com
Description
A 58-year-old woman was hospitalised with a relapse of thrombotic thrombocytopenic purpura (TTP). She was diagnosed with immune TTP 10 years ago and has had two previous relapses. Her first episode was treated with therapeutic plasma exchange (TPE) and high-dose steroids; two relapses, which occurred 3 years apart, were also additionally treated with rituximab. Rituximab treatment during the second relapse was discontinued early due to anaphylactic reaction to the third infusion. Previous acute complications of TTP included non-ST-elevation myocardial infarction. Following the last episode, the patient had persistent ADAMTS13 deficiency (activity less than 5%), but declined further immunosuppressive treatment.
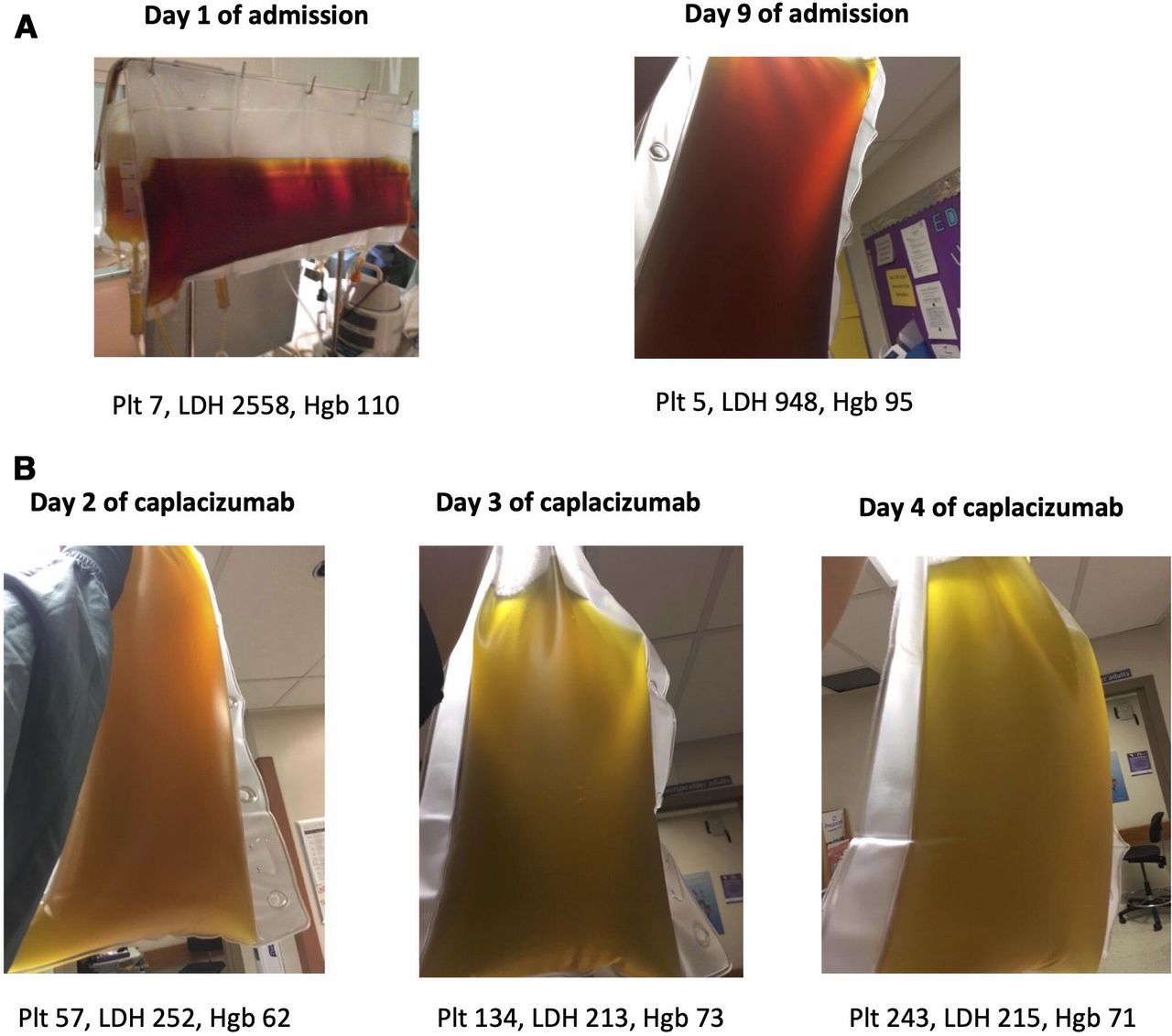
On admission, she had altered level of consciousness and required intubation. Admission bloodwork (day 1) revealed a platelet count of 7×109/L, haemoglobin 110 g/L, lactate dehydrogenase 2558 U/L (ULN 195 U/L), haptoglobin 0.03 g/L (normal 0.30–2.00 g/L) and indirect bilirubin 59 µmol/L (ULN 12 µmol/L). Blood film showed RBC fragmentation and ADAMTS13 activity was less than 1%. She had evidence of acute kidney injury (admission creatinine 192 U/L, ULN 102 U/L, baseline creatinine 51 U/L) and cardiac ischaemia (troponin 2.643 µg/L, ULN 0.4 µg/L). CT of the head did not reveal any acute pathology. TPE was initiated with solvent-detergent treated plasma and continued daily. The patient also received methylprednisolone 1 g daily for 3 days, followed by high-dose steroids. Rituximab treatment (4 weekly doses of 375 mg/m2) was delayed due to concerns about anaphylaxis, but eventually was administered on day 7, with desensitisation protocol. She tolerated rituximab but had no improvement clinically. There was also no improvement in her counts, haemolytic or organ damage markers (figure 1). Photographs of patient plasma on day 1 and 9 are shown in figure 2A, demonstrating significant haemoglobinaemia. Caplacizumab was requested through a compassionate access programme. The patient commenced caplacizumab 1 mg on day 10, using Caplacizumab Treatment for Acquired Thrombotic Thrombocytopenic Purpura (HERCULES) trial dosing protocol.1 Over the next few days, platelet count and lactate dehydrogenase improved dramatically (figures 1 and 2) and so did haemoglobinaemia (see figure 2B). The patient’s clinical condition also improved; she was extubated and discharged from intensive care unit on day 15 of admission (day 6 of caplacizumab). TPE was discontinued on day 15 (after 15 exchanges), and the patient was discharged home on day 17. Her renal function has normalised, and she did not have any permanent neurological deficits. There were no bleeding complications. The patient received her third and fourth doses of rituximab and completed a steroid taper as an outpatient. During steroid taper, she developed a local allergic reaction at the site of caplacizumab injections. As she was in clinical remission, doing well and eager to stop therapy, a decision was made to discontinue caplacizumab (after 65 days of therapy) and monitor her laboratory tests frequently. Her ADAMTS13 activity remained severely deficient, but she declined any further immunosuppression and to date has not relapsed.

Lactate dehydrogenase and platelet count over the course of patient’s admission with treatments shown. LD, lactate dehydrogenase; PLT, platelets; TPE, plasma exchange.
{kind=link}
{kind=link}
Photographs of patient’s plasma before (A) and after (B) caplacizumab treatment. Plt, platelets (109/L); LDH, lactate dehydrogenase (U/L); Hgb, haemoglobin (g/L).
This case report illustrates clinical and laboratory evolution of a patient with TTP refractory to standard of care therapies following addition of caplacizumab, adding to the few existing reports in the literature.2–4
Patient’s perspective
To have patience, faith and a caring doctor that did not give up on me and got me caplacuzimab that saved my life, gave hope for the future.
Learning points
Caplacizumab has been studied as initial therapy, but can also be rapidly effective in refractory TTP cases.
Caplacizumab had an acceptable safety profile with no bleeding complications in this critically ill patient.
Ethics statements
Patient consent for publication
Footnotes
Twitter @BrandonTse3
Correction notice This article has been corrected since published online first. The Competing Interest statement has been updated.
Contributors BT, MB and KP contributed to the acquisition and interpretation of data, writing the case report and review of the manuscript for publication. MB and KP managed the patient and contributed to the conception of the case report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KP declares honoraria for consulting and speaking from Ablynx/Sanofi and Shire/Takeda, participation in industry sponsored trials by Ablynx/Sanofi and Shire/Takeda.
Provenance and peer review Not commissioned; externally peer reviewed.