Article Text

Abstract
We outline a case of vaginal endometriosis in scar tissue located in the distal part of the anterior vaginal wall close to the urethra following repeated urogynaecological surgery. Our case presents a 45-year-old woman diagnosed with pelvic endometriosis in her youth. She underwent several vaginal surgeries due to pelvic organ prolapse, symptoms of stress incontinence and decreased urinary flow. One year after her most recent vaginal surgery, she developed a tender lump in the lower part of the anterior vaginal wall. A urethral diverticulum was suspected, but a diagnostic puncture and biopsy unexpectedly showed histologically verified endometriosis. As the cyst recurred, surgical excision of all visible endometriosis tissue was performed. After 3 years of follow-up, the patient remained without recurrence. This case illustrates the risk of atypical implantation of endometriosis related to repeated urogynaecological surgery and that treatment requires surgery with thorough removal of all visible tissues.
- obstetrics and gynaecology
- urological surgery
- vulvovaginal disorders
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Endometriosis is a chronic inflammatory disease defined by the presence of endometrial glands and stroma outside the uterine cavity. It is an oestrogen-dependent condition and, therefore, mainly present in the reproductive years. The prevalence is approximately 5% among fertile women. Pelvic endometriosis accounts for most cases with main localisations in ovaries and peritoneum (uterovesical fossa, ovarian fossa, pouch of Douglas).1
Vaginal endometriosis is predominantly described as being part of deep infiltrating endometriosis in the posterior fornix.2 However, endometriosis can also be diagnosed in more distal parts of the vagina, where it accounts for less than 1% of extrapelvic cases.3 This case draws attention to a rare location of endometriosis after repeated urogynaecological surgery in order to enable early diagnosis and appropriate treatment.
Case presentation
Our 45-year-old patient was referred to a urogynaecological clinic due to stress incontinence, decreased urine flow and nycturia. Despite the urine flow, she was planned for a tension-free vaginal tape (TVT) and anterior colporrhaphy. However, a cyst in the lower part of the anterior vaginal wall was identified, and surgery was postponed.
The patient had menarche at the age of 14, followed by regular periods without significant dysmenorrhoea. In her early 20s, she underwent laparoscopy two times: one diagnostic laparoscopy due to infertility without any signs of endometriosis, and one laparoscopy due to pain in which case peritoneal endometriosis was diagnosed. No deep endometriosis was found. She was treated with oral contraception for 1.5 years.
She had three spontaneous pregnancies and uncomplicated vaginal deliveries at the age of 25, 26 and 33. At the age of 34, she underwent laparoscopic sterilisation.
After her pregnancies, she developed symptomatic pelvic organ prolapse. During her 30s and early 40s, she underwent three vaginal operations: Manchester operation (including amputation of cervix and anterior colporrhaphy), anterior colporrhaphy and posterior colporrhaphy.
Her medical history included well-treated hypothyroidism and depression. There was no history of smoking or alcohol abuse. Body mass index was 30.9.
One year after the last vaginal surgery, she experienced pain and irregular periods with spotting. Vaginal examination revealed a tender process in the anterior vaginal wall at the level of the bladder neck.
Investigations
Ultrasonography revealed a cystic structure with suspicion of a urethral diverticulum. The T1-weighted images from an MRI scan showed a hyperintense 1.5 cm large cystic structure in the anterior vaginal wall, about 3 cm from the vaginal introitus, compatible with a blood-filled cyst (figure 1). The vaginal cyst was punctured, and a histological evaluation of a biopsy revealed endometriosis. No further treatment was initiated as the patient had no additional symptoms.
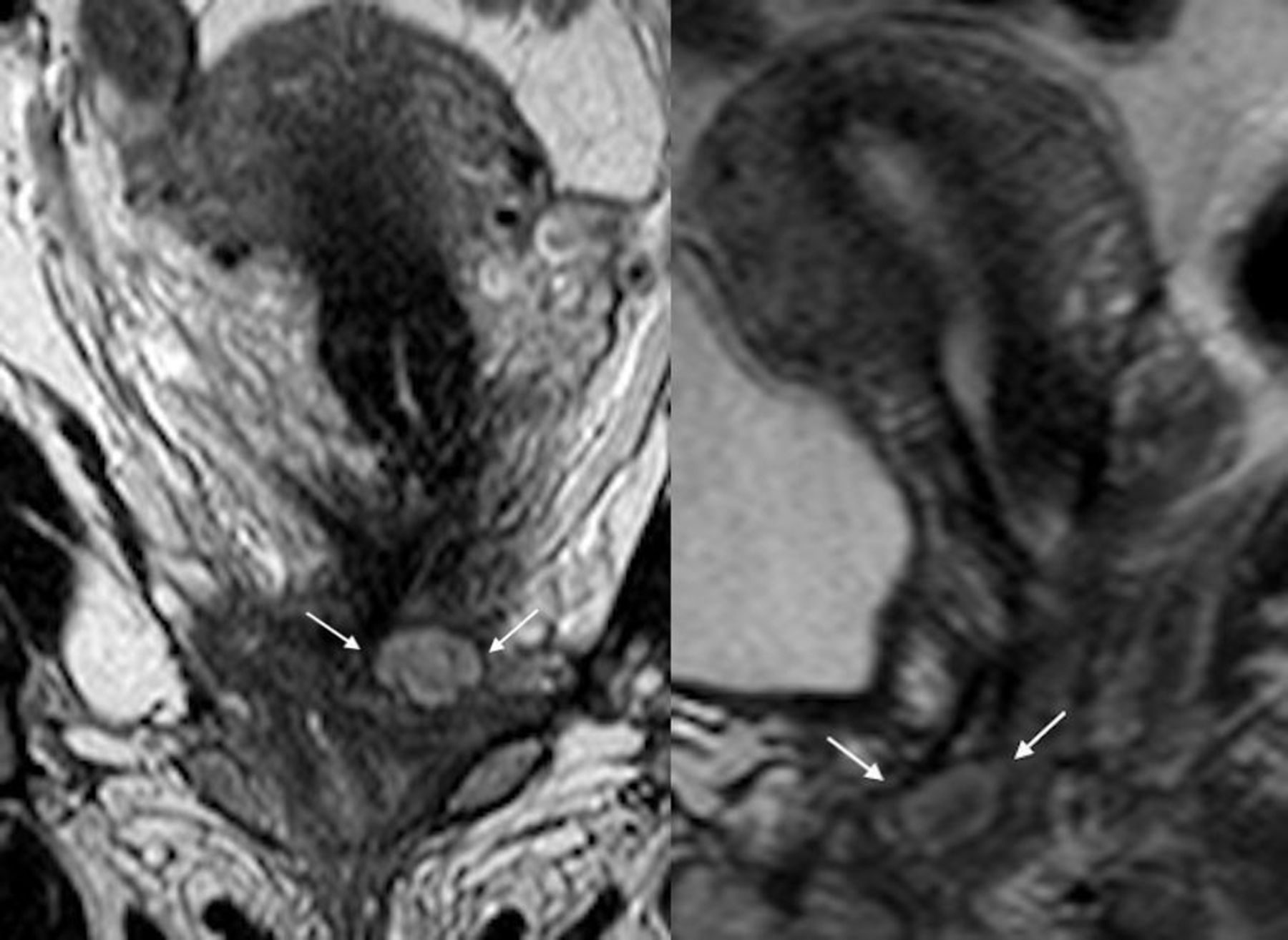
The endometriosis infiltration shown on MRI in coronal and sagittal plane.
Eight months later, a tender process was discovered at the same location, but without dyspareunia or bleeding. However, the patient still suffered from stress urinary incontinence and decreased urine flow.
The patient was then referred to The Endometriosis Centre at Copenhagen University Hospital, Rigshospitalet. Examination showed an infiltration in the lower third of the anterior vaginal wall, and ultrasonography disclosed a cyst close to the urethra with ground glass echogenicity measuring 1.5×2 cm close to the urethra. MRI confirmed the preliminary results and also visualised additional related smaller cysts.
Differential diagnosis
A urethral diverticulum or a benign cyst was suspected at first due to the patient’s urinary stress incontinence and concomitantly decreased urinary flow. To exclude another relevant differential diagnosis as Gartner duct cyst, Skene’s gland cyst and haemangioma, a biopsy was made.
Treatment
While awaiting the indicated surgical excision, the patient had developed cyclic pain from the process. It was treated with oral progestin (Provera 5 mg/day) for 1 month without success.
The surgery was initiated with a cystourethroscopy to ensure a normal urethra. The vaginal mucosa was opened in the lower part of the anterior wall. By sharp dissection, the vaginal cysts were excised from the location next to the bladder floor close to the urethra (figure 2). In total, three cysts were enucleated, the largest with a diameter of 2.5 cm. Classical endometriosis cyst content was found. All visible endometriotic tissues were removed. Finally, the patient had an intrauterine hormonal device (IUD).

{kind=link}
{kind=link}
Surgical excision of the endometriosis cysts from the anterior vaginal wall.
Outcome and follow-up
Histological examination confirmed the diagnosis of endometriosis. The IUD was removed due to migraine after 6 months.
Before the originally planned urogynaecological surgery, a follow-up MRI scan showed no recurrence of endometriosis, and the patient underwent anterior colporrhaphy and TVT with success. At 3 years of follow-up, the patient was still without recurrence of endometriosis.
Discussion
This case illustrates that endometriosis may implant in the distal part of the anterior vaginal wall after repeated urogynaecological surgery.
Vaginal endometriosis is usually found in the posterior fornix. The pathogenesis for this location is still debated. However, a widespread understanding is that it arises from the rectovaginal septum as part of deep endometriosis.4
Endometriosis in the distal part of the anterior wall of the vagina is rare, and the origin for this placement is unknown.
At the time of the examination of our patient, there were no similar cases to be found in the present research. However, while writing this case, an Australian case with a similar location of endometriosis has been reported.5 That case presents a patient with uncomplicated vaginal deliveries but without a history of gynaecological surgeries in contrast to our case.
Direct spreading of endometrial tissue and implantation during vaginal delivery should be considered, as endometrial tissue hypothetically could implant during delivery. But in that case, large numbers of vaginal endometriosis would be expected. Our patient’s symptoms occurred more than 10 years after her last delivery, which is a long time for asymptomatic proliferation of endometrial tissue. For these reasons, direct spreading is a less likely explanation.
A more plausible explanation is iatrogenic dissemination (implantation) after comprehensive vaginal surgeries (two anterior colporrhaphies) prior to a diagnosis of endometriosis. Especially, the Manchester operation including amputation of cervix and anterior colporrhaphy could lead to iatrogenic dissemination of endometrial tissue. This assumption is based on the fact that scar endometriosis is well known6 7 and theories of endometrial tissue spillage during surgery have been described before. A large Swedish register study found a hazard risk of 1.8 for general pelvic endometriosis in women, who had had a previous caesarean section, compared with women with only vaginal delivery.8 This corresponds with the general understanding, that the risk of postsurgical endometriosis does not correlate to a preoperative diagnosis of endometriosis. In case stories, the anticipation is that postoperative endometriosis is found after laparoscopic supracervical hysterectomy with morcellation of the uterus.9 10 In a case–control study with 464 women undergoing hysterectomy (277 of them had a laparoscopic supravaginal hysterectomy (LSH) with morcellation; 187 had a transvaginal or abdominal hysterectomy without morcellation), a rate of 1.4% of postoperative endometriosis was found after hysterectomy, with no difference between the LSH group and the control group.11 Our patient was diagnosed with peritoneal endometriosis nearly 30 years before the latest vaginal surgery. Based on previous case stories, iatrogenic implantation due to repeated vaginal surgery is the most likely explanation for this rare location, even though the mentioned case–control study did not find such a connection.
The symptomatology of endometriosis depends on the location of the endometrial tissue, but commonly dysmenorrhea, chronic pain, fatigue and infertility are described.12 The broad symptomatology and delayed diagnosis can lower the health-related quality of life significantly for the patients.13
This patient had a tender distal vaginal swelling and occasional irregular bleeding and associated pain. In the beginning, the pain was unspecific but became cyclic. The main complaints from the patient were urinary incontinence (stress type) and decreased urinary flow. Therefore, a urethral diverticulum or a benign cyst was suspected at first. Under usual conditions, a TVT would not be planned for patients with urinary incontinence and decreased urinary flow, but in this case, the decreased flow was most likely due to obstruction by the endometriotic nodule in the lower anterior vaginal wall. Because of the rare location, endometriosis was not suspected initially, even though the patient was diagnosed with endometriosis in the past. To our knowledge, no studies have shown that patients with previously described endometriosis have a higher risk of scar endometriosis than the background population.
The evidence for treating extragenital endometriosis is limited and mainly published in case reports and case series.14 In this case, the conservative hormone treatment of the vaginal endometriosis infiltration was unsuccessful with limited relief of pain. Only surgical excision removed the obstruction.
Despite advanced surgery, recurrence of parietal endometriosis lesions occurs in 5% of cases in the literature.15 However, recurrence incidence varies as it is non-uniformly defined in the literature.16 The present patient underwent one surgery with removal of all visible endometriotic tissues with no recurrence reported after 3-years of follow-up.
Learning points
The symptomatology of endometriosis is extensive.
Endometriosis must be suspected in patients presenting with a tender swelling in the distal part of the vagina.
Atypical implantation of endometrial tissue is a possible risk after repeated urogynaecological surgery.
Time from surgery to the onset of symptoms can extend over years.
Treatment of atypical endometriosis requires surgery with thorough removal of all visible tissue.
Ethics statements
Footnotes
Contributors SP and JJK were involved in the patient’s care and proposed the case. AEC drafted the manuscript. SP, DH and JJK contributed to the paper by proofreading a number of drafts and suggesting corrections. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.