Article Text

Abstract
A 54-year-old woman with insulin-requiring type 2 diabetes mellitus presented with acute shortness of breath and drowsiness on a background of polydipsia, weakness and significant weight loss. One year ago, she had decided to stop her insulin and other medications and adopt lifestyle modifications instead. Initial emergency department (ED) blood samples were highly lipaemic and appeared strawberry pink. She was eventually diagnosed with diabetic ketoacidosis (DKA) with severe hypertriglyceridaemia, intubated for airway protection, and managed with fluid resuscitation and intravenous insulin to good effect. We share an uncommon DKA presentation at the ED. History was limited as the patient was drowsy and minimally communicative. Physical examination was unremarkable. Blood investigations were also delayed in view of the need for additional centrifugation. These contributed to a paucity of information in the acute setting and resulted in a diagnostic challenge.
- resuscitation
- diabetes
- lipid disorders
- adult intensive care
- diet
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
This report describes an uncommon presentation of diabetic ketoacidosis (DKA). The patient was brought into the emergency department (ED) by her husband in a drowsy and minimally communicative state and could only provide limited history. Physical examination was also unremarkable. Blood investigations taken at the ED were severely lipaemic and appeared strawberry pink. The high lipaemic index appeared to cause derangements in point-of-care tests (POCT). Laboratory tests also took up to three times the usual duration to return, and multiple parameters had to be rejected in view of the additional centrifugation required. These delays and paucity of information resulted in a diagnostic challenge. The patient was eventually diagnosed with DKA with severe hypertriglyceridaemia (HT), intubated for airway protection, and managed with fluid resuscitation and intravenous insulin.
When faced with abnormally coloured blood in a critically ill patient, differentials to consider include cyanide poisoning, dyshaemoglobinaemia (eg, carboxyhaemoglobin and methaemoglobinaemia), lipaemia and drug overdose. Severe lipaemia may affect the findings and accuracy of POCT and laboratory tests. A review of the effects of lipaemia on POCT and blood tests will be discussed.
Case presentation
A 54-year-old woman with a medical history of type 2 diabetes mellitus (T2DM) was brought in with an acute onset of shortness of breath and drowsiness. One year before presentation, she had stopped her metformin and subcutaneous insulin against medical advice and started adopting lifestyle modifications, including regular exercise and a modified diet comprising mostly of fruits and salads with intermittent fasting from 09:00 to 21:00 daily. She had also started taking traditional Chinese medications, specifically fish oil, black garlic and lingzhi. Six months in, she started experiencing polydipsia, back and thigh aches, and significant intentional weight loss of 27% (from 52 kg to 38 kg). Her husband also started to notice atrophy of her leg muscles associated with a slow gait and difficulty climbing stairs. She was otherwise well and did not have any other known medical conditions. She did not have a family history of hyperlipidaemia. There was no history of drug overdose, self-harm or exposure to smoke or fumes.
On presentation, she was noted to be dehydrated and drowsy with a Glasgow Coma Scale of 6 (E1V1M4). The patient was also noted to be in sinus tachycardia and tachypnoea with a heart rate of 125, a respiratory rate of 28 and a blood pressure of 157/113. She was otherwise afebrile and saturating well on room air. The patient appeared cachexic and malnourished. Physical examination was otherwise unremarkable with equal and reactive pupils, no pink skin or bright red lips, and no signs of pancreatitis.
Investigations
Blood samples were lipaemic and appeared strawberry pink (figures 1 and 2). POCT arterial blood gas and electrolytes were performed with an Abbott i-STAT System using CG4+ and CHEM8+ test cartridges, respectively, which revealed a high anion gap metabolic acidosis (HAGMA; anion gap 16.5) attributed to lactic acidosis and ketosis (serum ketones 16.47 mmol/L and lactate 3.47 mmol/L) with inadequate respiratory compensation and hyperkalaemia (table 1, S/N 1). In view of concerns of POCT accuracy in the setting of profound lipaemia, a second POCT was done 30 min later, which suggested hypokalaemia instead (table 1, S/N 3). The electrolytes laboratory panel taken at the same time as the first POCT performed via indirect ion-selective electrochemistry (ISE) and was eventually reported only 3 hours after first presentation (compared with 1 hour in a typical sample) in view of need for extensive centrifugation. This revealed HAGMA (anion gap 44.0, delta gap 1.6) with normokalaemia (Serum glucose 31.5 mmol/L, urea 7.2 mmol/L, serum osmolality 312 mOsm/kg (calculating formula: 2×(Na)+(glucose)+(urea); usual range 270–285)) (table 1, S/N 2).
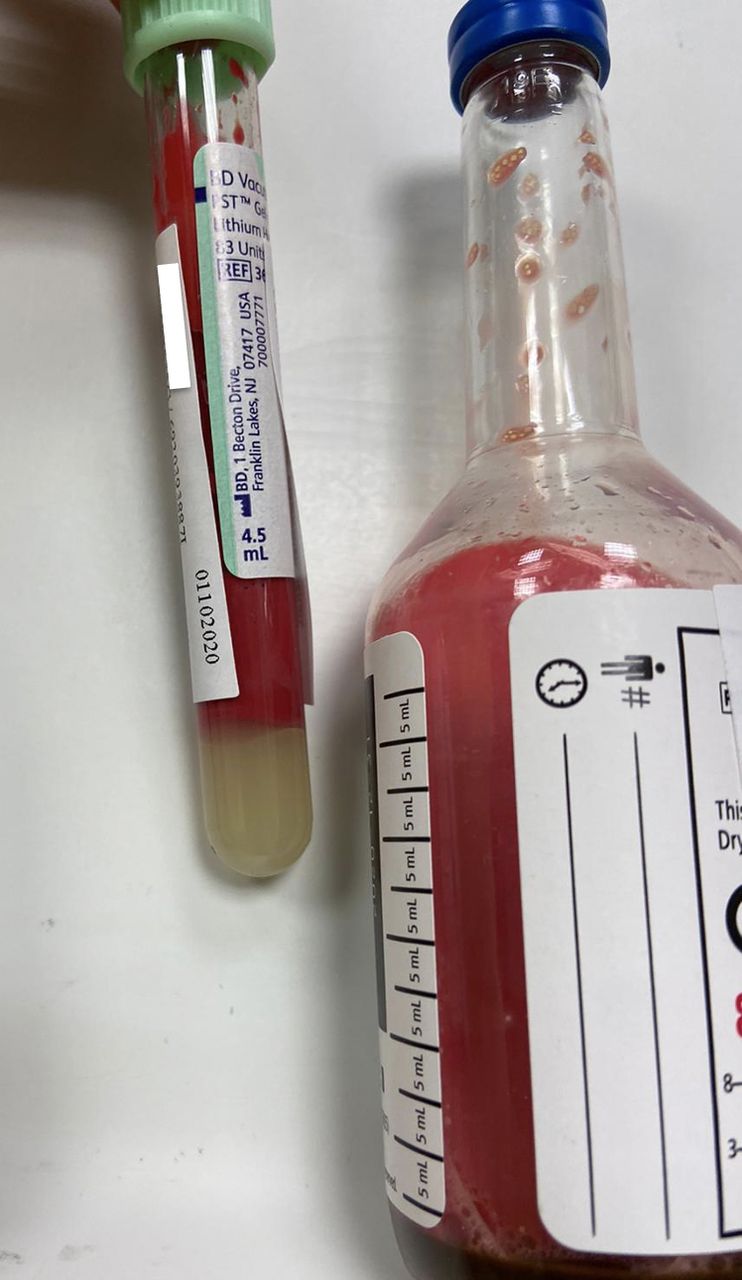
Clinical photograph of this patient’s blood taken on presentation in the emergency department (colours not digitally edited).

{kind=link}
{kind=link}
Demonstration of patient’s blood separating into two distinct layers over time. The distinct opaque supernatant is caused by the precipitation of a high concentration of triglycerides in the blood.
Summary table of pertinent blood gas and electrolyte investigations taken in the emergency department
Several tests were also rejected as the blood samples that remained suitable for analysis were insufficient after discarding the lipid supernatant. The remaining laboratory investigations returned at various timings from 30 min to 3 hours post venipuncture and demonstrated severe hyperlipidaemia and HT with a total serum cholesterol of 47.07 mmol/L (usual range 0.00–5.20 mmol/L) and serum triglycerides (TG) of 267.66 (0.00–2.20 mmol/L). (The patient’ high-density lipoprotein and serum low-density lipoprotein were 0.28 mmol/L (1.00–1.60 mmol/L) and 3.85 mmol/L (0.00–3.30 mmol/L), respectively.) There was no significant biochemical evidence of pancreatitis. Her glycated haemoglobin was 8.2%. Serum troponin, liver function tests, thyroid function tests, creatine kinase, paracetamol and salicylate levels, carboxyhaemoglobin, and calcium, magnesium and phosphate levels returned normal. A urine full examination, microscopic examination (UFEME) returned positive for glucose 4+, ketones 4+ and proteins 4+. An ECG was done, which demonstrated sinus tachycardia and no signs of hyperkalaemia or hypokalaemia. Chest X-ray (CXR) and abdominal X-ray as well as CT brain imaging were grossly normal.
Differential diagnosis
In general, the differentials of acute dyspnoea can be broadly classified into cardiovascular, respiratory and metabolic causes. Cardiovascular causes include acute coronary syndrome, cardiac tamponade and heart failure. Respiratory causes are more extensive and can be further subdivided into upper and lower airway aetiologies—upper airway causes comprising largely of obstructive pathologies, such as anaphylaxis and foreign body ingestions, and lower airway causes, including pneumothorax, pulmonary embolism and pulmonary infections. Examples of metabolic causes include, but are not limited to, metabolic acidosis (lactic acidosis and uraemia), thyrotoxicosis and drug overdose.
The patient had a significant medical history of T2DM requiring insulin, which she was non-compliant to. This resulted in symptoms of polydipsia, weight loss and muscle atrophy. On examination, she also appeared cachectic and malnourished. Blood tests demonstrated hyperglycaemia, ketosis, lactic acidosis and HT, and her UFEME returned positive for glucosuria, ketonuria and proteinuria. These led us to the eventual diagnosis of severe DKA with HT secondary to medication non-compliance and sepsis of unknown origin. Of note, there were no other complications of poorly controlled diabetes noted, such as diabetic kidney disease (serum creatinine 36 µmol/L) and ischaemic strokes, and no complications of HT, such as pancreatitis, lipaemia retinalis and cerebral oedema.1–3Starvation ketoacidosis was a consideration in view of the patient’s history of dietary restriction, weight loss and muscle wasting. However, such patients tend to have a low-to-normal blood glucose reading at presentation.4 In our opinion, her weight loss and muscle wasting were more likely contributed by catabolic states observed in DKA.
Treatment
Although investigation results were delayed, the patient was managed expediently according to the tenets of critical care in a ‘first principles’ approach, and a definitive airway was secured in view of the patient’s drowsiness. After the patient was stabilised, she was reassessed and additional corroborative history was taken from her spouse. She was subsequently admitted to the intensive care unit (ICU) where she was treated as for severe DKA and sepsis precipitated by Escherichia coli bacteriaemia. She was resuscitated with 7 L of fluids within the first day of admission and started on intravenous meropenem and a continuous insulin infusion. Her lactic acidosis resolved within day 2 of admission (0.71 mmol/L from 3.47 mmol/L at admission) while her ketoacidosis resolved over 3 days. She was successfully weaned off intravenous insulin infusion on day 4 to subcutaneous insulin, and extubated and transferred out of the ICU on the same day. As of the time of transfer, she had been started on statins and fibrates and her HT and hypercholesterolaemia had improved. Her blood cultures returned positive for pansensitive E. coli while her urine cultures returned negative. A CXR and contrasted CT of her abdomen and pelvis was performed, but returned negative for any obvious source of infection.
A multidisciplinary approach was adopted, and the patient was referred to endocrinology and renal medicine for further management, insulin titration and chronic outpatient follow-up of her diabetes. She was also reviewed by the hospital dietician for dietary and nutrition management, as well as occupational therapists and physiotherapists for rehabilitation and muscle recovery. The patient was educated on her condition and the importance of medication compliance to mitigate risks of recurrence.5 Her DKA and HT improved throughout her inpatient stay and she was eventually discharged well on day 18 of admission. As of the time of discharge, her total serum cholesterol and TG had downtrended from 47.07 mmol/L to 11.69 mmol/L and 267.66 mmol/L to 0.78 mmol/L, respectively.
Outcome and follow-up
The patient remains asymptomatic and well at the time of writing. She has been compliant to her insulin injections and other diabetes medications. Outpatient follow-up investigations performed 1 month after discharge returned normal (total serum cholesterol 5.22 mmol/L, TG 0.45 mmol/L, random urine protein <0.04 mg/dL and UFEME negative for glucose and ketones). She did not experience any other complications of poorly controlled diabetes, such as neuropathy and retinopathy. She will continue to be on routine outpatient follow-up with endocrinology for her diabetes management.
Discussion
In this case study, the likely precipitating factors are medication non-compliance and intercurrent sepsis. Although the patient’s low-carbohydrate diet is unlikely the cause of her DKA, there have been case studies reported of such diets triggering severe euglycaemic DKA when sodium-glucose transporter-2 inhibitors are concomitantly taken as the resultant glucose deficiency not only generates the weight loss so desired by dieters, but also precipitates lipolysis and extreme metabolic states.6–10 The aetiology behind the altered mental state witnessed in this patient and other cases of severe DKA is ascribed predominantly to metabolic acidosis in the presence of hyperosmolarity and sepsis.10 11 Indeed, in this case, both biochemical derangements were present (pH 6.8, serum bicarbonate 4.5 mmol/L, base excess −29.1 mEq/L and serum osmolality 312 mOsm/kg).
During the initial management of this patient, key challenges faced included delays in recognising that the patient’s abnormal blood colour was caused by severe lipaemia, concerns regarding POCT accuracy in lipaemic samples, and delays in blood investigations due to the extensive centrifugation required. Differentials of bright pink venous blood include cyanide and carbon monoxide poisoning, hypothermia, dyshaemoglobinaemias and lipaemia. Other aetiologies of abnormally coloured blood include methaemoglobinaemia (may appear brownish) and sulfhaemoglobinaemia (may appear darker red with a bluish hue). The most common causes of lipaemic blood samples include parenteral administration of lipid emulsions, such as propofol, and total parenteral nutrition and HT.12–14 Other rarer causes include familial hypercholesterolaemia, adult lymphoblastic leukaemia and lipoprotein lipase (LPL) deficiency.15–17 The proposed mechanism behind HT in DKA is insulin deficiency, resulting in lipolysis and the release of free fatty acids (FFAs) from adipose tissues. The release of glucagon in response to starvation also contributes in part to the subsequent lipolysis. The FFAs released are subsequently transported to the liver and potentiate the production of very-low-density lipoprotein, resulting in HT.
As of time of writing, this is the second case of severe HT in the presence of DKA secondary to poorly controlled T2DM. A previous case was described of a 19-year-old man who presented with a triad of acute pancreatitis, HT and DKA secondary to undiagnosed T2DM.18 Cases reported of HT from T1DM have moderate HT with peak TG levels ranging from 11.5 mmol/L to 163.4 mmol/L (compared with a peak serum TG level of 267.66 mmol/L in this patient), are often the first presentation of diabetes, and are more commonly male patients with a normal pH on presentation.1–3 19 20 HT increases blood viscosity, which may lead to blood vessel occlusion to the pancreas and brain, resulting in complications of acute pancreatitis and cerebral oedema, respectively.1 20–22 The acute management of HT in DKA revolves around the management of DKA proper, as insulin increases LPL activity which, in turn, metabolises chylomicrons and serum TG.20 23 Although most cases in literature experienced normalisation of TG levels within 2 weeks of insulin treatment alone,1 this patient was also prescribed statins, fibrates and omega-3 fish oil in view of her extremely high TG levels and presumed benefit with minimal risks or contraindications. In severe cases, plasmapheresis is a therapeutic option and has been described to reduce TG levels by up to 70% in a single session, decreasing the overall length of stay.18 24 25
The patient’s calculated anion gap of 44 (from the electrolytes laboratory panel taken at presentation) was too high to be attributed to ketoacidosis alone and there were no other possible causes of HAGMA identified (eg, uraemia, toxicological causes, such as methanol, salicylates and carbon monoxide). This observation may be attributed to pseudohypobicarbonataemia (serum bicarbonate falsely low) during the analysis of the lipaemic blood samples. Lipaemia is a known source of laboratory errors, particularly pseudohyponatraemia and pseudohypobicarbonataemia,1 26–28 and a case using ISE has been reported.29 Further discussion, which concerns light scattering and enzymatic assay interferences, is beyond the scope of this paper.19 26 27 29 ISE is used in most large hospital biochemical laboratories for electrolyte analysis, including ours. Interestingly, the Abbott i-STAT uses an enzymatic system dependent on photometric analysis, which has been tested in vitro with intralipid to lipid levels as high as 111 mmol/L, with no significant interference found.27 29 However, there is no available data on higher concentrations (our patient had a serum TG of 267.66 mmol/L), and recommendations are to ultracentrifuge such samples, which defeats the purpose of a POCT and may not be feasible in the acute emergency setting.
The management of lipaemic samples is institution-dependent, with most laboratories opting to reject tests known to be erroneous in the presence of lipaemia.30 Centrifugation of samples prior to testing, however, is effective and should be employed to minimise errors.26 Taking the laboratory result as accurate (based on previous studies on the laboratory management of lipaemic samples and use of centrifugation), the POCT results appear to demonstrate pseudohyponatraemia and pseudohyperchloraemia (table 1), although pseudohypochloraemia is more commonly reported in HT.1 Potassium levels also varied from 3.0 mmol/L to 6.0 mmol/L in POCT samples compared with 3.6 mmol/L in the laboratory result. We postulate that varying levels of haemolysis may have caused the observed variations in potassium levels. This is because although the POCT machine and cartridges were accurately calibrated, venipuncture was straightforward and there were minimal delays in running specimens, lipaemia itself is often associated with haemolysis. This phenomenon is attributed to alterations in the lipid composition of erythrocyte membranes in the presence of HT, resulting in increased fragility.19 31
The comparisons above are done solely between the two POCT results and one laboratory blood result taken at admission and therefore must be interpreted with discretion. Although there are several studies published in biochemistry and laboratory journals on the effects of lipaemia on laboratory blood results,12 26 30 there is a paucity of information on POCT results. Guidelines recommend checking potassium levels prior to insulin treatment as insulin causes an intracellular shift of potassium, which may result in hypokalaemia and life-threatening arrhythmias.6 11 32 As time is required to obtain accurate laboratory results (as in this case), POCT results may, therefore, be required to guide actual treatment and management in the emergency setting. As such, it is imperative that additional studies be done on the effects of lipaemia on POCT results, although potentially challenging to conduct.
Patient’s perspective
I used to follow a strict diet and intermittent fasting regime. These were from some Youtube videos and websites I read online. I also started to take some traditional Chinese medicine instead of my medications as I believed it would help my diabetes. I have been feeling occasional bouts of thirstiness for the past year, especially during my holiday trips in November 2019 to Japan and January 2020 to Australia, but did not think it would be related to diabetes. Since my discharge, I have been taking my medications regularly and have started checking my blood glucose regularly. I am now also on regular follow-ups with my diabetes doctor and nurse educator, who have been helping me to adjust my insulin dosages. My husband has been encouraging me to eat more carbohydrates, and I have gained 4 kg kg since my discharge from hospital. I am thankful to have survived, and grateful to the doctors and nurses who have cared for me during my hospitalisation.
Learning points
Severe hypertriglyceridaemia (HT) is an uncommon complication in patients with diabetic ketoacidosis.
The finding of abnormal coloured blood in critically ill patients may provide a clue to the underlying aetiology.
A differential of strawberry pink blood is HT, which, in turn, may cause laboratory errors, such as pseudohyponatraemia and pseudohypobicarbonataemia.
Despite the potential for lipaemic blood specimens to delay and interfere with biochemical analyses, it is important to initiate resuscitation and supportive measures for such critically ill patients according to first principles.
Ethics statements
References
Footnotes
Contributors TXZT, SHCL and JK conducted the literature review and directed the conception and design of this study. TXZT, SHCL and JK carried out the acquisition, analysis and interpretation of data, and subsequently drafted the manuscript. TXZT, SHCL and JK provided critical revision of the manuscript for important intellectual content. All authors meet the criteria for authorship stated in the Uniform Requirements for Manuscripts Submitted to Biomedical Journals, and have made substantial contributions to all of the following: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; (3) final approval of the version to be published; and (4) agreement to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.