Article Text

Statistics from Altmetric.com
Description
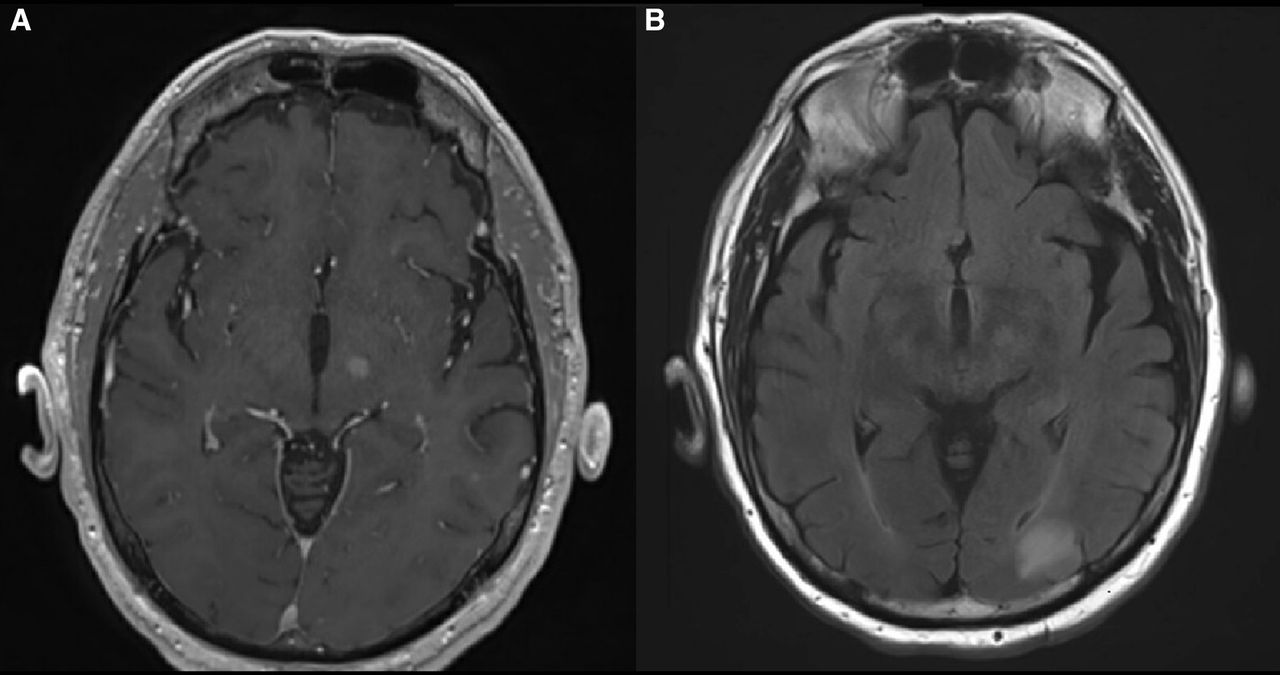
A 72-year-old man presented with a 4-week history of uncontrolled flowing movements of the right upper extremity (RUE) and right lower extremity (RLE). Examination was significant for right haemichorea–haemiballism with RUE more pronounced than RLE (video 1). Initially, he was able to suppress these movements for brief periods of time; however, over the previous 2 weeks, the movements progressed in frequency and intensity. He started high-dose steroids with mild improvement. Brain MRI showed multiple supratentorial lesions including a 0.7×0.7 cm lesion in the inferior left thalamus or subthalamus (figure 1). MRI of the spine showed a contrast enhancing soft-tissue mass measuring 2.2×2.8×3.0 cm in the L5 laminectomy bed. Positron emission tomorgraphy (PET) scan showed additional hypermetabolic mediastinal and peripancreatic lymph nodes, subcutaneous chest wall nodule and soft-tissue mass along left femur. Biopsies of the chest wall mass returned as a high-grade undifferentiated pleomorphic sarcoma.

{kind=link}
Axial T1 postcontrast (A) and T2 FLAIR (B) MRI demonstrating a 0.7×0.7 cm lesion in the inferior aspect of the left thalamus, in the vicinity of the subthalamic nucleus.
Haemiballismus has historically been attributed to lesions of the contralateral subthalamic nucleus (STN), but more recent studies have identified pathology in a variety of other locations, particularly other basal ganglia structures.1 2 The differential diagnosis includes ischaemic or haemorrhagic stroke, hyperglycaemic, traumatic brain injury, central nervous system infections, brain metastases, paraneoplastic haemiballism and other rare processes that disrupt thalamic pathways that regulate motor function. Haemichorea-haemiballism secondary to a metastatic lesion in the basal ganglia is rare and has only been described in a handful of case reports. Acquired haemiballismus in the setting of malignancy should prompt careful consideration of metastases within the basal ganglia and STN or ischaemic stroke. A thorough evaluation will include an MRI, biopsy when indicated, assessment of standard metabolic parameters, complete and detailed neurologic examination and testing for onconeural antibodies when feasible. Unlike paraneoplastic haemiballismus, haemichorea–haemiballism secondary to a metastatic or ischaemic injury is unlikely to be associated with the presence of onconeural antibodies.3
In the case of this patient, his haemichorea–haemiballism was attributed to a metastatic lesion in the region of the subthalamus, as identified on MRI. Diffusion-weighted imaging was not consistent with stroke or vascular injury. The STN is a key structure in the indirect pathway of basal ganglia motor function. The STN and other basal ganglia nuclei regulate the firing pattern of the globus pallidus interna. Injury to the STN can lead to the development of haemiballism/haemichorea.1 2 Unfortunately, the lesion within the left thalamus was not amenable to resection. In an attempt to palliate his symptoms before starting systemic therapy, it was recommended that all intracranial metastases be treated with fractionated stereotactic radiosurgery. He required anaesthesia for all radiation treatment in order to control his haemichorea–haemiballism and oxygen saturation. Unfortunately, his symptoms progressed rapidly and efforts to medically palliate involuntary movements were only moderately successful without full sedation. Shortly after receiving his first dose of fractionated radiotherapy (800 cGy), he developed altered mental status, dysarthria and rhabdomyolysis, and was subsequently transitioned to hospice at the request of his family.
Patient’s perspective
On admission, our father was hopeful that he would improve with treatment and was highly supportive of the academic contribution and presentation of his unique case. He found encouragement in the idea that others could learn from his situation, and he saw this as a positive perspective in the setting of an otherwise discouraging diagnosis. As his symptoms continued to worsen, we were very saddened to see his condition deteriorate. For both our father and our family, quality of life was highly important. Over a short period of time, our father had lost the ability to consistently and meaningfully interact with us. It was difficult to watch him be in so much distress and unable to control his movements, to the point where he was exhausted and could not find relief without sedation. Having to immobilise and sedate him for treatment was emotionally challenging, especially for our mother, who expressed great empathy and concern for his autonomy. She expressed that he ‘would not have wanted to continue like this, especially if he could not get better. This was not the life he would want.’ As our father developed further complications, we made the difficult decision to transition to hospice care, and he passed away shortly thereafter. Though we all acknowledge the emotional difficulty of discussing his passing, we wanted to honour his final wishes and fully support publication of his case.
Learning points
Haemichorea–haemiballism and haemiballism are rare hyperkinetic movement disorders. Haemiballism is characterised by large amplitude movements involving the proximal limb while chorea is characterised by smaller amplitude movements of the the distal extremities.
The differential diagnosis for acquired haemiballismus includes: acute ischaemic or haemorrhagic stroke, metabolic disturbance, traumatic brain injury, structural basal ganglia lesions/malignancy, vascular malformations, central nervous system infections and demyelinating plaques. Unlike immune-mediated paraneoplastic causes, metastatic lesions are unlikely to be associated with antibodies and are more likely to present unilaterally.
Metastatic lesions in the subthalamic nuclei causing haemiballismus are rare and have only been described in a few case reports.
Ethics statements
Footnotes
Contributors ALHA was involved in direct patient care, treatment delivery, interacting with and obtaining consent from the family, and conception and writing of the case report. TLS was involved in direct patient care, interacting with and obtaining consent from the family, recording the videos, editing the videos and conception and writing of the case report. MEG was involved with the conception and writing of the case report. SRJ was involved direct patient care, editing the videos and conception and writing of the case report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.