Article Text

Statistics from Altmetric.com
Description
A 22-year-old woman was presented to the emergency department of the tertiary care centre with abdominal pain, continuous dribbling of urine and haematuria for 3 days. She had a history of obstructed labour 4 days ago, which was managed at a peripheral centre leading to the vaginal delivery of a dead male child. She was primigravida and had not visited for any antenatal care previously. At presentation, her blood pressure was 100/60 mm Hg, pulse rate was 100/min and had a mild fever. She was given a brief resuscitation, after which a vaginal examination was performed which revealed a tear in the anterior vaginal wall. Her urethra could not be localised for the placement of Foley’s catheter. Therefore, an urgent MRI of the pelvis (figures 1 and 2) was ordered to look for genito-urinary injuries and fistula. MRI of the pelvis was perfomed after distending the vagina and anal canal with inert jelly. MRI (figure 1) showed a defect in the anterior wall of the bladder with leakage of urine into the extraperitoneal space (anterior vesical space, vesicovaginal space and perineum). Another defect (figure 2A,B)was seen in the lower anterior vaginal wall communicating with the perineum. Subchondral increased signal intensity on short tau inversion recovery sequence images (figure 2) suggestive of bone marrow oedema was seen in bilateral pubic symphysis associated with mild superior displacement of left pubic bone and oedema in adjacent muscles. Surgical anastomosis in two layers was done for both anterior vaginal and anterior bladder defects with the placement of suprapubic and perivesical drains. The patient recovered well, and her drains were removed on the 15th postoperative day. Conservative management was done for pubic symphysis injury using a pelvic binder.
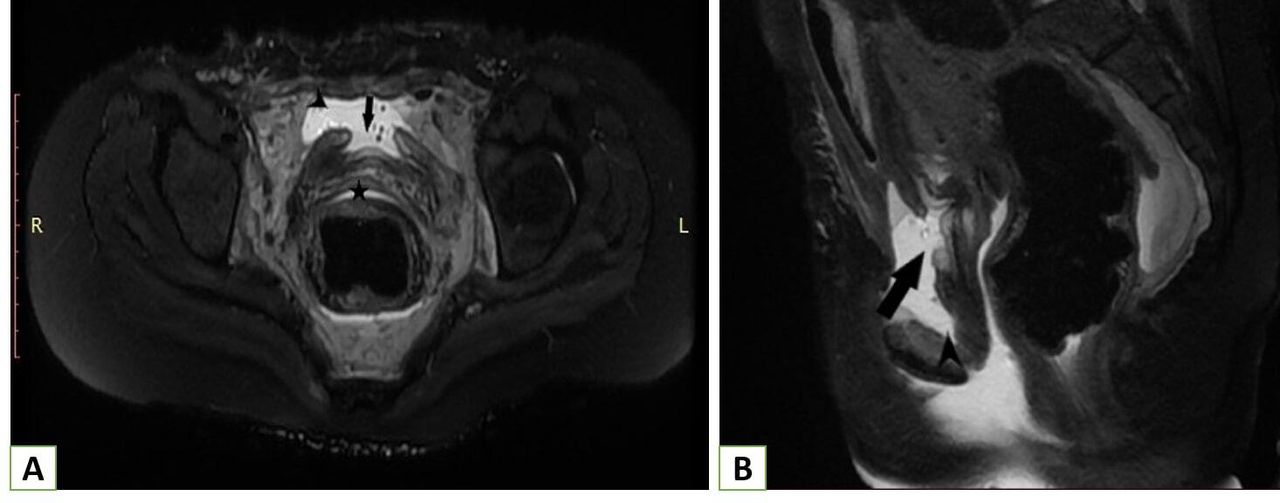
MRI of the pelvis. T2 weighted fat-saturated in axial (A) and sagittal (B) planes show a defect in the anterior urinary bladder wall (black arrow) with extraperitoneal fluid collection (arrowhead). Note the normal upper part of the vagina (star).

{kind=link}
{kind=link}
MRI of the pelvis. T2 weighted fat-saturated in axial (A), sagittal (B) planes and stir coronal (C) images show a defect in the lower anterior vagina wall (black arrow) with a normal uterus and upper two-third of the vagina (yellow arrow). Subchondral bone marrow oedema was observed at pubic symphysis with mild superior displacement of the left pubic bone (blue arrowhead). Associated muscle oedema is present in bilateral obturator muscles (white arrow). Note the normal urethra (star) in image B.
Obstructed labour is not uncommon in developing countries where primary healthcare is not readily available in outreach areas. Moreover, people from low socio-economic status are not aware of the importance of regular antenatal check-ups and prefer that women give birth at home under the supervision of untrained attendants. Complications of obstructed and neglected labour include fetal death, shock, sepsis, uterine rupture, urinary bladder rupture, genitourinary and rectouterine fistula.
Anterior bladder wall rupture in the absence of uterine rupture is exceedingly rare, especially in primigravida.1 2 Possible causes of anterior bladder wall rupture could be due to urine retention in the urinary bladder during labour and external fundal pressure as the labour was unsupervised. There are also few case reports of abdominal massage-related bladder rupture and spontaneous bladder rupture during labour.3 4
Patients with obstructed labour are usually haemodynamically unstable and immediately admitted for emergent exploratory laparotomy. However, in cases of delayed presentation with urinary leak and haematuria, with prior history of obstructed or prolonged labour, an urgent MRI of the pelvis should be performed. On MRI, along with evaluation of genitourinary injuries, the presence of pubic diastasis and pelvic bone injuries can also be detected. Prior imaging will guide in planning of the surgery and adequate rehabilitation of the patient.
Patient’s perspective
I developed continuous lower abdominal pain and dribbling of urine mixed with blood after the delivery while I was admitted to a local hospital. They referred me to the hospital in the city for further treatment. Hereafter local examination, I underwent MRI in which they found that my urinary bladder was ruptured due to which my urine was continuously leaking. I was taken up for immediate surgery. Now, after 1 month of surgery, I am completely fine. I am very thankful to all the doctors and their team who had given me good treatment and care.
Learning points
Persistent urinary leakage and haematuria following prolonged or obstructed labour should raise the suspicion of urogenital injuries.
If such patients are haemodynamically stable, an MRI of the pelvis should beperformed to look for the extent of urogenital injuries and the presence of pelvic bone fracture/diastasis.
Extraperitoneal anterior urinary bladder wall rupture is exceedingly rare in a primigravida with obstructed labour, especially without associated uterine rupture.
Ethics statements
Acknowledgments
The author would like to thanks Mr P B Singh for coordinating in image formatting.
Footnotes
Contributors PS has written the manuscript and collected the images.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.