Article Text

Statistics from Altmetric.com
Description
We report the case of a 69-year-old male patient, observed for vesiculobullous lesions involving the oral mucosa (figure 1), trunk and extremities. There were also more evolved lesions with crusted surface and erythematous cicatricial plaques covered by milia cysts.

Vesiculobullous lesions involving the oral mucosa.
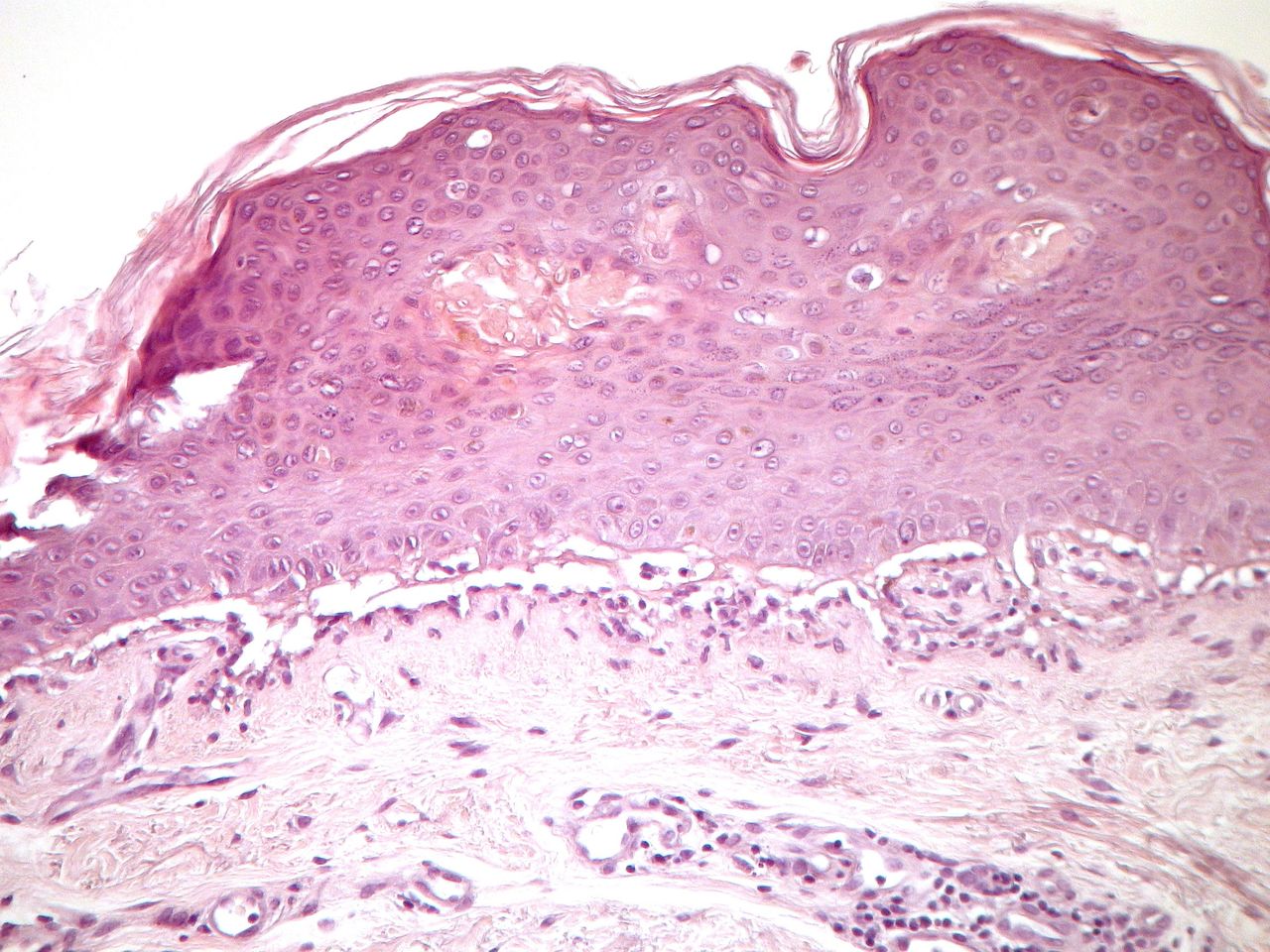
Histology revealed a cell-poor subepidermal blister (figure 2), and direct immunofluorescence showed linear deposition of IgG and C3 along the dermoepidermal junction.

{kind=link}
{kind=link}
Histology showing a subepidermal detachment with scant inflammatory infiltrate (H&E ×100).
ELISA detected circulating antibodies against collagen VII, confirming the diagnosis of epidermolysis bullosa acquisita (EBA).
He was initially medicated with methylprednisolone 24 mg and dapsone 50 mg every day in combination with topical therapy. For lack of response, dapsone was replaced by azathioprine, initially 50 mg once a day, then 50 mg two times a day and then reduced to the initial dose due to side effects. Due to the ineffectiveness of the therapy and the side effects associated with corticosteroids and azathioprine, he initiated rituximab therapy, having performed four cycles with slight improvement and transient stabilisation of the clinical picture, without reaching complete remission.
EBA is a rare acquired, mucocutaneous, subepidermal, autoimmune blistering disease, which results in vesicle and bullae formation on the skin and erosions on the mucous membranes.1–5 EBA can evolve with cicatricial mucosal involvement, leading to respiratory, ocular and/or digestive sequelae with important morbidity.1–3 It usually appears in adulthood (with a median age of 50 years), with no known predilection to sex.1–3 Clinically, it can present with numerous phenotypes, though the most common are the mechanobullous and inflammatory variants; EBA includes various distinct clinical manifestations resembling bullous pemphigoid, Brunsting-Perry pemphigoid or cicatricial pemphigoid.1–4 There is an association with HLA-DR2 and the patients have autoantibodies against collagen VII, an integral component of anchoring fibrils responsible for attaching the dermis to the epidermis.1–3 It may be associated with other diseases, such as diabetes mellitus, thyroiditis, Crohn’s disease, systemic lupus erythematosus, lymphomas, pernicious anaemia and autoimmune thrombocytopenia.1–3 The importance of the differential diagnosis of this entity with other subepidermal autoimmune bullous dermatoses, such as bullous pemphigoid, linear adult IgA dermatosis and bullous systemic lupus erythematosus, is highlighted.1–4 Diagnosis is established by having a consistent clinical presentation, direct immunofluorescence and autoantibodies against collagen VII.1–3 Once the diagnosis is established, however, it is challenging to find optimal treatment for the patient.1–5 Multiple drugs have been used in the treatment of EBA, resulting in varying degrees of response; the most frequently reported agents include systemic corticosteroids, anti-inflammatory and immunosuppressive agents.1–5 Currently, treatment is often unsatisfactory; however, some success has been achieved with colchicine, dapsone, azathioprine, photopheresis, plasmapheresis, infliximab, rituximab and intravenous immunoglobulins.1–5 EBA, especially in its classic form, is characterised by poor response to immunosuppressive therapies.1–5 There have been developments in newer treatment modalities that have achieved some success.1–5 Rituximab, an anti-CD20 monoclonal antibody, alone or in combination with other agents, showed potential to induce long-term remission in EBA resistant to other treatments.1–5
Learning points
Few cases of epidermolysis bullosa acquisita (EBA) have been described in the literature.
Diagnosing EBA is often difficult because of the variety of clinical presentations that may overlap with other blistering diseases, such as bullous pemphigoid and cicatricial pemphigoid.
Rituximab was shown to be effective in this case of EBA previously resistant to other therapies.
Ethics statements
Footnotes
Contributors SRM (first author): acquisition and analysis of data, planning, conducting, conception and design of the article, as well as revision and final approval. IC: acquisition of data and final approval. JCC: acquisition of data, revision and final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.