Article Text

Abstract
To describe the case of a 48-year-old Japanese female patient with more than two decades of experience in jazz dance instructor returning to work after simultaneous bilateral total hip arthroplasty (SBTHA). We provided her with a tailored postoperative physical therapy programme considering her preoperative activity level and skills using three-dimensional motion analysis for guidance. The patient returned to jazz dance instruction 8 months after undergoing SBTHA, and her disease-specific quality of life assessment score at 1-year postsurgery was almost perfect. Use of three-dimensional motion analysis helped facilitate our assessment of whether her hip angle was within the acceptable range for teaching the compound movements necessary in jazz dance, but her preoperative experience was crucial in determining her full-scale participation in jazz dance. At present, 7 years since the surgery, the patient is able to continue jazz dancing, the THA component remains stable.
- physiotherapy (rehabilitation)
- physiotherapy (sports medicine)
- osteoarthritis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
It is not uncommon for young patients who have undergone total hip arthroplasty (THA) to wish to return to their preoperative occupations and sports activities.1 Evidence on which sports should be allowed as well as when and at what frequency they are permissible is lacking.2 3 For this reason, surgeons largely rely on their experience and judgement to determine an individual patient’s readiness to return to sports after THA. Ollivier et al reported that 16.3% of postoperative THA patients participated in dance activities.4 However, whether it is safe to dance after THA is a concern for both patients and physical therapists. Many patients who want to return to sports after THA are anxious about such complications as dislocation, wear and loosening.4 5 In addition, a higher percentage of respondents report fear and doctor’s recommendation rather than postoperative pain and lack of interest in sports as reasons for not engaging in sports activities.4 6 It is, therefore, necessary for patients to collaborate with their surgeon to eliminate their anxiety about dislocation and be reassured that they can perform sports-related movements through rehabilitation aimed at helping them return to their sports after THA.
On the other hand, previous studies comparing simultaneous bilateral THA (SBTHA with staged THA have shown that SBTHA is safer and leads to earlier improvements in hip flexion range of motion (ROM) and daily activities.7 8 Furthermore, Yoshii et al found that, compared with unilateral THA, SBTHA resulted in significant improvement in the disease-specific quality of life (QOL) of patients after THA based on the Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire (JHEQ).9 Movement analysis data for hip angles less than 90° have been reported for hula dancing and classical ballet,10 whereas those for hip angles greater than 90° are lacking. Patients who wish to achieve more advanced dance movements require a higher ROM of the hip joint, muscle strength, and movement in postoperative rehabilitation.11
In this report, we describe the case of a patient who returned to work as a jazz dance instructor after SBTHA and her recovery of lower extremity function, walking ability and QOL. Simultaneously, we describe movement instruction using a three-dimensional (3D) motion analysis device. To the best of our knowledge, this is the first study to show a patient’s successful return to jazz dance instruction after SBTHA.
Case presentation
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. The CARE checklist was used for this case report.12
The patient was a 48-year-old Japanese female jazz dance instructor (height, 156.0 cm; weight, 53 kg; body mass index, 20.9 kg/m2) in 2013. At the time of her surgery, she had 23 years of jazz dance experience and was running a dance studio, teaching students and organising and performing in musicals. She had bilateral hip pain from 2003 and was diagnosed with acetabular dysplasia. Her pain did not improve despite conservative treatment, and she was diagnosed with bilateral acetabular labral tears. She underwent arthroscopic labral repair of the right hip in 2010 at another hospital due to her reduced dance performance and that of the left side in 2011. However, because of the progressive deformity of her hip joint and the more severe pain she was experiencing, she could no longer perform deep hip flexion movements in jazz dance. She consulted the orthopaedic surgery department of our hospital to discuss a treatment plan, and she was diagnosed with bilateral advanced osteoarthritis, for which the surgeon recommended SBTHA (figure 1). She was briefed by the surgeon on the risks and other possible complications involved in performing THA. She consented to these in writing and underwent cementless SBTHA at our hospital in 2013 (figure 2). The operation was performed bilaterally using a transtrochanteric approach.13 The cementless titanium alloy stem (neck, 0 mm; K-MAX Q Hip Stem), AMS HA shell (multihole; outer diameter, 46 mm), 2-methacryloyloxyethyl phosphorylcholine-grafted liners (Aquala) and cobalt–chromium–molybdenum alloy femoral ball (28 mm) used in this study were all obtained from KYOCERA Medical (Japan). The basic dislocation position was forced flexion of the hip joint or combined hip extension and external rotation. The patient’s acceptable hip joint ROMs after SBTHA based on the intraoperative hip angles were 130° of flexion, 25° of extension, 70° of abduction, 30° of right adduction, 20° of left adduction, 90° of external rotation and 30° of internal rotation.

Preoperative X-ray of the patient’s hips showing bilateral osteoarthritis. Centre edge angle, right hip/left hip: 12°/18°; sharp angle, right hip/left hip: 46°/44°; acetabular head index, right hip/left hip: 62.5%/58.3%.

X-ray of the patient’s hips following simultaneous bilateral total hip replacement. (A) One-week postsurgery. (B) Seven years postsurgery.
Treatment
Physical therapy was started on the third day after THA. Physical therapy during hospitalisation was performed 5 days a week, once a day, for 60 min. The patient was able to perform daily activities without a cane 21 days postsurgery and subsequently discharged home. Outpatient physical therapy was started 28 days postsurgery and performed once a week for 80 min each time. She hoped to be able to perform sufficient lower extremity flexion in the long sitting position and grand plié in the second and parallel position. We therefore performed physical therapy with the goal of increasing her ROM in hip flexion, abduction and external rotation as well as enabling her to fully support her bodyweight within the ROM of the hip joint.
Outcome and follow-up
Two months after surgery, she started practising steps and turns without hip flexion of greater than 90° under our supervision. She returned to work as a dance instructor 2 months postsurgery. However, her work then consisted mainly of verbal dance lessons and office work. At 7 months postsurgery, the surgeon allowed her to practise dance movements with greater than 90° of hip flexion, but she was anxious about hip dislocation this time. To reduce her anxiety and provide her with a safer hip flexion angle, we used a 3D motion analysis device (UM-CAT II, 180 Hz; UNIMEC, Japan) for motion guidance. The reflex markers were placed at the anterior superior iliac spine, greater trochanter of the femur, and centre of the anteroposterior diameter on the lateral side of the knee joint. As this device could display data in real time, we could tell her the hip flexion angle required in dancing and daily life activities (figure 3). Hence, she was able to safely perform the movements she wanted to after surgery (figure 4). At 8 months postsurgery, she was able to jump on the spot and make soft landing movements (figure 5). She acquired safe dance movements 8 months postsurgery and returned to full-time work as a jazz dance instructor. Her JHEQ results at 1-year postsurgery showed that she had a high QOL with a hip dissatisfaction score of 3 mm and a total score of 81/84 points bilaterally (mental status, −3 points). The patient’s physical function tests were measured at 3 weeks, 6 months and 8 months postsurgery, and the results are shown in table 1.

Assessment of the patient’s hip flexion mobility during movement using 3D motion analysis. (A) Squatting position. (B) Flexion of the lower limb in the long sitting position. Hip flexion: (A)100°, (B)119°. Marker: (5) anterior superior iliac spine, (6) greater trochanter of the femur, (7) centre of the anteroposterior diameter on the lateral side of the knee joint. 3D, three dimensional.

Progress in the patient’s grand plié in the second and parallel position. (A) Pre-THA. (B) Three months postsurgery. (C) Eight months postsurgery. Hip flexion (passive/dynamic): (B) 110°/72°, (C) 130°/119°. THA, total hip arthroplasty.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
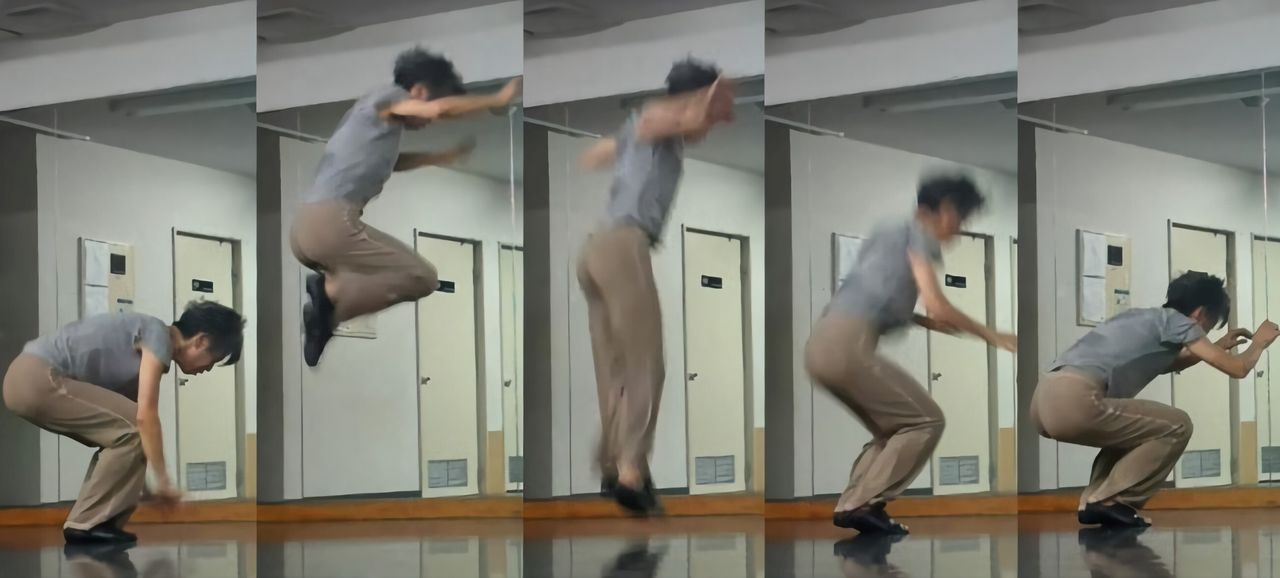
The patient’s jumps and soft landings at 8 months postsurgery.
Patient’s recovery progress
Discussion
This is the first study to investigate the dynamic kinematics of the hip joint required for jazz dance movements in a patient after SBTHA and to show progress in recovery of lower extremity function. The patient’s hip ROM improved to the intraoperative ROM at 8 months postsurgery. The maximum flexion angles of the hip joint during movements using 3D motion analysis were 100° for squatting down during dancing and 119° for flexion of the lower leg from the long sitting position. Jazz dance is a dance genre that incorporates elements of ballet. Research has shown that the average hip flexion and abduction in the splits position in ballet are 133.2° and 32°, respectively.14 The patient was able to achieve a wide ROM in the hip joint because she had a high degree of flexibility in the soft tissues around the hip joint due to her years of dance experience and because she was able to rigorously follow a self-training programme.
Although a wide range of dances are recommended after THA,2 many people give up on dance genres that involve high-impact on the hip joint and deep hip flexion, such as jazz dance, after surgery15 and considerable caution should be exercised when engaging in these activities.16 In the present case, dislocation associated with hip flexion was of particular concern. Studies on impingement of the component, one of the causes of THA dislocation, have shown that impingement was present in more than half of dislocated cases.17 18 Data have also shown that patients who participate in high-impact activities involving the hips and those who are less active do not differ in the frequency of dislocation.19 In the present case, the surgeon asked the patient about the hip angle she needed for dancing before performing the surgery. The surgeon also determined the acceptable range of hip angles during rehabilitation after ensuring that impingement of the component would not occur during surgery. Sharing of this information between the surgeon, therapist, and patient helped reduce her anxiety about dislocation. By using 3D motion analysis to practise movements involving hip flexion of greater than 90°, we were able to safely coach her on dislocation prevention and reduce her anxiety. In addition, she was able to jump vertically and had soft landing movements at 8 months postsurgery. In various movements in ballet, ‘beauty’ (softness), rather than vigour, is emphasised; in such landing movements as the sissonne fermée, it is customary to land softly from a state of plantar flexion of the ankle joint.20 Therefore, we considered that the patient’s landing technique was not newly acquired after THA and rather honed through her years of experience in jazz dance. As a result, her JHEQ score at 1-year postsurgery was almost perfect and her hip satisfaction level was high. Seven years have passed since the surgery, and she continues to be active without pain, dislocation, or wear but still needs to be observed.
The results of this case of an instructor with many years of dance experience are not likely to be applicable to all postoperative THA patients who wish to engage in jazz dancing. A patient should have considerable experience in a given high-impact sport before undergoing THA to be able to resume participating in it after surgery.21 However, in this case report, we were able to prove the need for patients, surgeons and physical therapists to share information and for medical professionals to consider each patient’s level of sports activity and skills. Our findings also indicate that use of 3D motion analysis helps reduce patients’ anxiety and allows for safer movement instruction.
Patient’s perspective
When I watch a video of myself dancing 14 years ago, when I started to have hip pain, I can see that I was very flexible at that time. However, I never thought that I would be using a cane after 7 years. I can still vividly recall that the pain in my hip joint was enough to change my life in the blink of an eye. The changes in my life are the way other people look at me and the financial issues. As I walked with a limp, my reputation with the people around me quickly diminished, and eventually I stopped receiving requests for dance work and became poor. It has been 7 years since my surgery, and I still occasionally do choreography that requires a deep hip bend, like crouching on the floor. Sometimes I feel the stiffness in my hip joints, but I enjoy it without straining myself. Now, based on my own experience, I lecture classes on how to use the body in a way that does not strain the joints. I will never forget the joy of being freed from the mental and physical stresses of that time by the surgery. My life is now much happier.
Learning points
Information sharing and collaboration among patients, surgeons, and physical therapists is important to return to more hip-impacting sports.
The use of three-dimensional motion analysis is a useful tool in reducing patient anxiety about treatment and ensuring patient recovery after simultaneous bilateral total hip arthroplasty (THA).
Patients after THA need to have considerable preoperative experience before they can resume high-impact sports such as jazz dancing.
Ethics statements
Acknowledgments
A part of this report was presented at the 55th Annual Meeting of the Japanese Association of Rehabilitation Medicine, Japan, in 2018. We would like to thank the surgeon for explaining the ROM of the hip joint during the surgery and the condition of the hip joint postsurgery. We are grateful to our patient for sharing her sentiments and allowing us to include her statement in this report.
References
Footnotes
Twitter @Mizo_yasu
Contributors YM was responsible for writing and drafting the manuscript. TU and HK were responsible for reviewing, guiding and editing the final draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.