Article Text

Statistics from Altmetric.com
Description
An 88-year-old woman presented to our hospital due to an 18-hour history of worsening central chest pain. She had a dual-chamber pacemaker due to second-degree Mobitz type II atrioventricular block implanted 10 years ago. Her risk factors included hypertension and hypercholesterolaemia. Her admission ECG showed a ventricular paced rhythm with ST changes consistent with ST-elevation myocardial infarction (STEMI) according to Smith-modified Sgarbossa criteria (SMSC) (figure 1), leading to activation of the primary percutaneous coronary intervention (pPCI) pathway. An urgent coronary angiogram showed a proximally occluded left anterior descending artery, and pPCI of the culprit vessel was performed, with restoration of Thrombolysis in Myocardial Infarction (TIMI) II flow (figure 2). A bedside echocardiogram showed akinetic anterior and anteroseptal walls with severely impaired left ventricular systolic function. The post-pPCI ECG showed paced rhythm with resolution of the ST-segment changes. Unfortunately, 2 days later she developed cardiogenic shock, suffered a cardiac arrest and died.

(A) Patient’s ECG on arrival meeting the Smith-modified Sgarbossa criteria for STEMI. (B) The diagnostic algorithm proposed for diagnosing STEMI in RVPR/LBBB. (C) The original and the Smith-modified Sgarbossa criteria. AMI, acute myocardial infarction; LBBB, left bundle branch block; PCI, percutaneous coronary intervention; RVPR, right ventricular paced rhythm; STEMI, ST-elevation myocardial infarction.

{kind=link}
{kind=link}
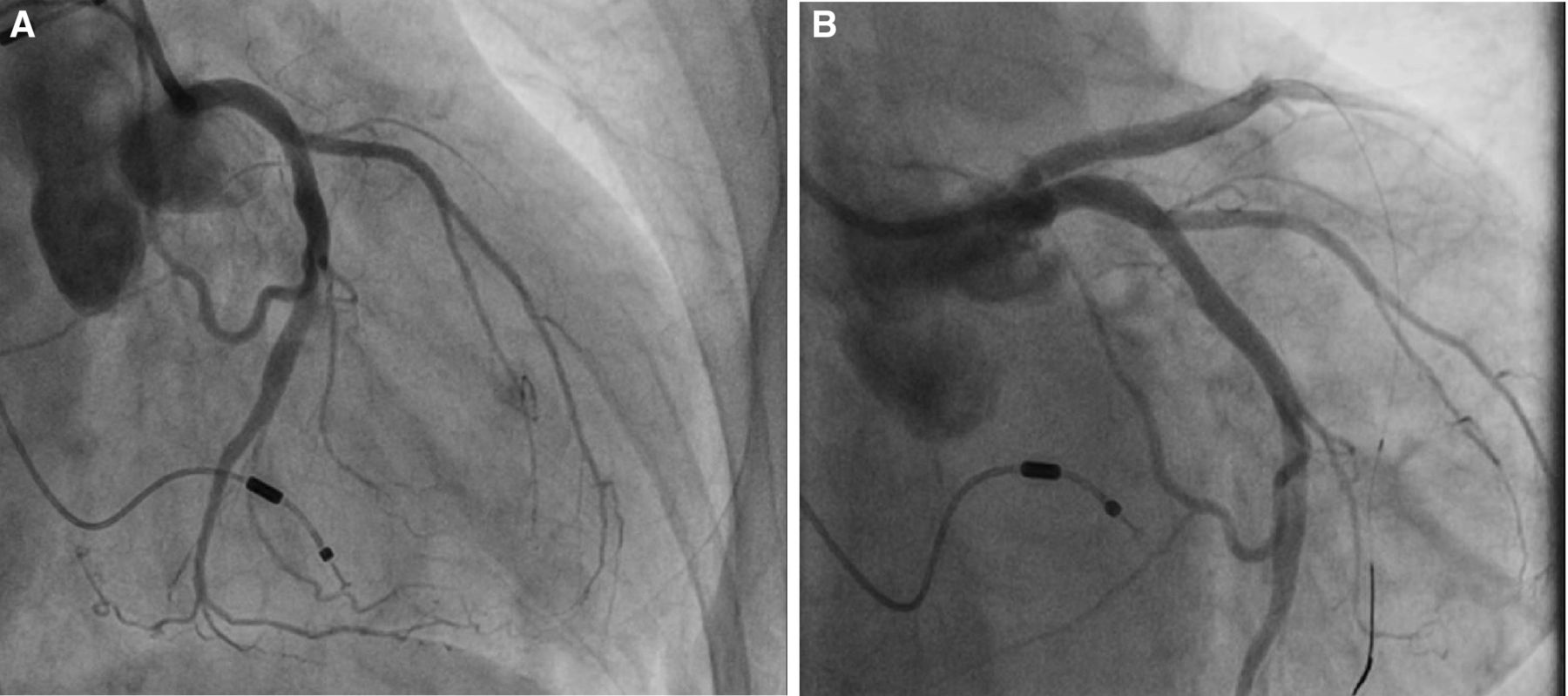
Coronary angiogram showing an occluded left anterior descending artery (A) with restoration of flow following primary percutaneous coronary intervention (B).
It is believed that a left bundle branch block (LBBB) pattern on the ECG can complicate the electrocardiographic diagnosis of acute myocardial infarction (AMI) due to the presence of repolarisation abnormalities hiding ST-segment changes consistent with myocardial ischaemia. Right ventricular paced rhythm (RVPR) results in an intraventricular conduction delay similar to that seen with LBBB. As is the case with LBBB, it is a common misconception that one cannot identify STEMI in a patient with a ventricular paced rhythm.
The original Sgarbossa criteria (OSC) have traditionally been used to assist with the diagnosis of STEMI in patients with LBBB and RVPR,1 and are the following:
Concordant ST-segment elevation ≥1 mm for leads with a predominantly positive QRS complex—score of 5.
Concordant ST-segment depression ≥1 mm in leads V1, V2 or V3—score of 3.
Excessively discordant ST-segment elevation ≥5 mm in leads with negative QRS complexes—score of 2.
A total score of ≥3 suggests that the patient is having an AMI. However, although the specificity of the OSC is good, their sensitivity is low and cannot be applied to rule out an acute coronary event. Smith et al2 derived the SMSC using angiographic outcomes and defining excessively discordant ST elevation in proportion to the preceding S-wave if greater than one-fourth its depth (ST/S ratio >0.25), rather than using an absolute value (≥5 mm), proposing a modification to the OSC third criterion and the diagnostic algorithm (figure 1).2 A recent multicentre retrospective study showed that the SMSC are far more sensitive than the OSC for the diagnosis of AMI in the presence of RVPR (sensitivity of 81% vs 56%) while maintaining high specificities (84% vs 90%).3 The sensitivity of the SMSC is even higher if criterion 2 from the OSC is extended out to V1–V6 (instead of only V1–V3).3 These findings dispel the notion that it is not possible to diagnose AMI in patients with RVPR and LBBB, many of whom would be candidates for timely reperfusion therapy.
Learning points
Right ventricular pacing with left bundle branch block (LBBB) morphology can complicate ECG interpretation in the diagnosis of acute myocardial infarction (AMI), but careful analysis of it is still important, as it can occasionally be diagnostic.
The Smith-modified Sgarbossa criteria are significantly more sensitive than the original Sgarbossa criteria for the diagnosis of AMI in paced rhythm/LBBB.
If a patient meets the Sgarbossa or Smith-modified Sgarbossa criteria in an appropriate clinical context, prompt cardiac catheterisation laboratory activation is appropriate.
Ethics statements
Footnotes
Contributors VP has collected the clinical information for this case and supervised the writting up of the case as the senior author. AV reviewed the literature and wrote the discussion part of this case. Both authors worked together to format the manuscript appropriately.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.