Article Text

Statistics from Altmetric.com
Description
A 28-year-old male patient presented with a broken filling on tooth 26. The patient reported that the filling had dislodged and has been refilled multiple times previously. On further enquiry, he complained of tenderness on the left cheek, left nasal blockage and postnasal drip occurring sporadically for over a year. The patient had visited physicians and otorhinolaryngologists and has been prescribed multiple courses of antibiotics with no effect. At the time of dental visit the patient was on Augmentin 625 mg as prescribed by the physician. He was also given the option of surgical treatment of the chronic maxillary sinusitis by the physician, but he was not interested in this course of action.
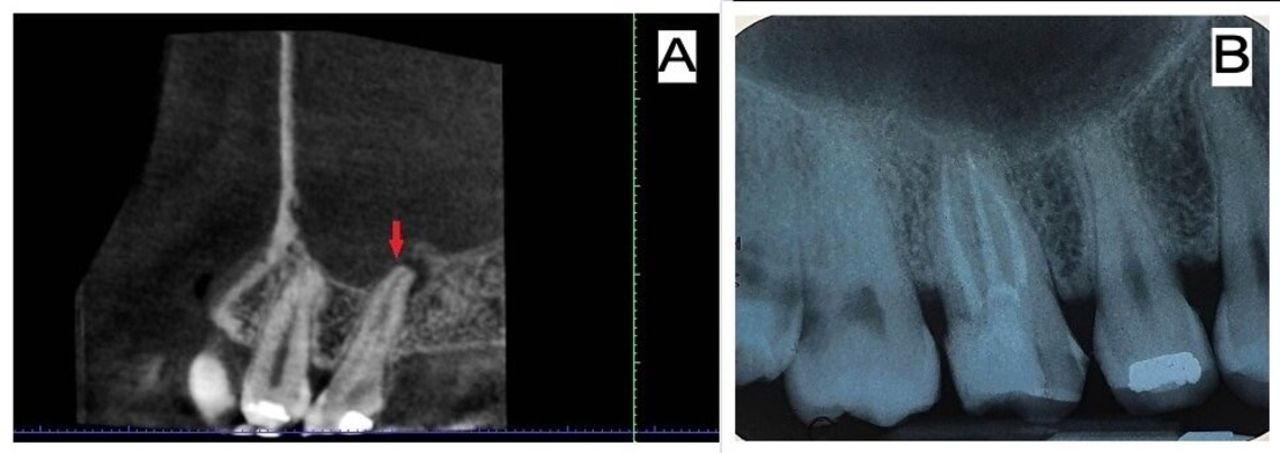
On oral examination there was a fractured disto-occlusal tooth coloured filling extending subgingivally on tooth 26 with food impaction. Tooth 26 was tender on percussion and showed no response to electric pulp test. Diagnostic periapical radiograph of tooth 26 did not show anything conclusive, so cone beam CT (CBCT) with voxel size of 150 µm was advised. Three-dimensional CBCT imaging increases the accuracy of detecting periapical lesions and any abnormalities of the nasal and paranasal sinuses when compared with conventional imaging modalities.1 Axial and coronal sections of the CBCT images revealed total opacification of the left maxillary sinus, as seen in figure 1A,B. The sagittal section of CBCT showed that the root apices of tooth 26 protruded into the maxillary sinus through a perforation in the thin cortical boundary of the maxillary sinus (figure 2A). A diagnosis of necrotic tooth 26 resulting in odontogenic maxillary sinusitis was made. A conservative and non-surgical treatment approach was considered. Thus, endodontic treatment of tooth 26 was advised.

(A,B) Coronal and axial sections of preoperative cone beam CT showing total opacification of the left maxillary sinus (arrow), while the right sinus appears normal. L, left; R, right.

{kind=link}
{kind=link}
(A) Sagittal slice of cone beam CT showing the infected root apex of tooth 26 (arrow) encroaching into the sinus space. (B) Postobturation Intra-oral Periapical Radiograph of tooth 26.
Following administration of buccal infiltration anaesthesia and isolation with rubber dam, access cavity preparation was done on tooth 26. Mesiobuccal, distobuccal and palatal canals were detected. Initial working length was determined with an apex locator (Root ZX, J Morita), which was 21 mm in the palatal and distobuccal canals and 20 mm in the mesiobuccal canal. Chemomechanical preparation was completed using ProTaper and Hyflex CM rotary files (Coltene Whaledent, Altstätten, Switzerland). Irrigation during mechanical instrumentation was done using 2.5% sodium hypochlorite. Calcium hydroxide intracanal medicament was placed into the root canals and the tooth was filled temporarily with Cavit. In the next appointment after 2 weeks, irrigation was done with 2 mL of 17% EDTA solution, followed by a final rinse of 5 mL saline solution. Obturation was completed by cold lateral condensation technique using AH Plus sealer (figure 2B) and a composite restoration was done on tooth 26.
At 1-month follow-up appointment, the patient had complete resolution of symptoms of sinusitis and there was no discomfort in relation to the endodontically treated tooth. Following this a full coverage restoration was fabricated and placed on tooth 26. A simple yet thorough endodontic treatment was able to sort the patient’s dental as well as sinus issues which have been troubling him for over a year. This case thus enforces and highlights to the clinician the importance of eliciting proper case history and using appropriate investigative tools such as CBCT. Similar treatment outcomes have been achieved in various case reports in the literature using non-surgical endodontics.2 3 Thus following this protocol will contribute to accurate diagnosis and treatment, which will provide swift relief to patients.
Patient’s perspective
I never imagined that a visit to the dentist would result in the successful treatment of my blocked nose and sinus issues. I had gone to my dentist to get a pesky filling sorted. The dentist was very thorough in her queries and was soon to figure out why I was having repeated bouts of sinus pain, and bad phlegm in my mouth when I slept. Multiple visits to the ENT resulted in me having lots of anti-biotics and even considering surgery for my sinus issues. But a simple and painless root canal treatment fixed my sinus and dental concerns. I will always be grateful to my dentist for her patient listening and her excellent treatment. Now I believe dental treatment is not only about fixing teeth but the body also.
Learning points
Otorhinolaryngologists should consider dental aetiology in cases of persistent unilateral maxillary sinusitis and refer patients for further dental consultations to achieve early diagnosis and effective treatment.
Odontogenic maxillary sinusitis is most commonly associated with infected maxillary molars due to the close anatomical proximity between root apices and sinus boundaries.
Cone beam CT has different advantages including high contrast resolution, elimination of superimposition of anatomical structures and reduced radiation exposure compared with multislice CT and so should be considered in such cases.
Ethics statements
Footnotes
Contributors LLV was responsible for diagnosis and treatment of the case. AB was involved in treatment planning and follow-up of the manuscript. AB was involved in drafting of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.