Article Text

Statistics from Altmetric.com
Description
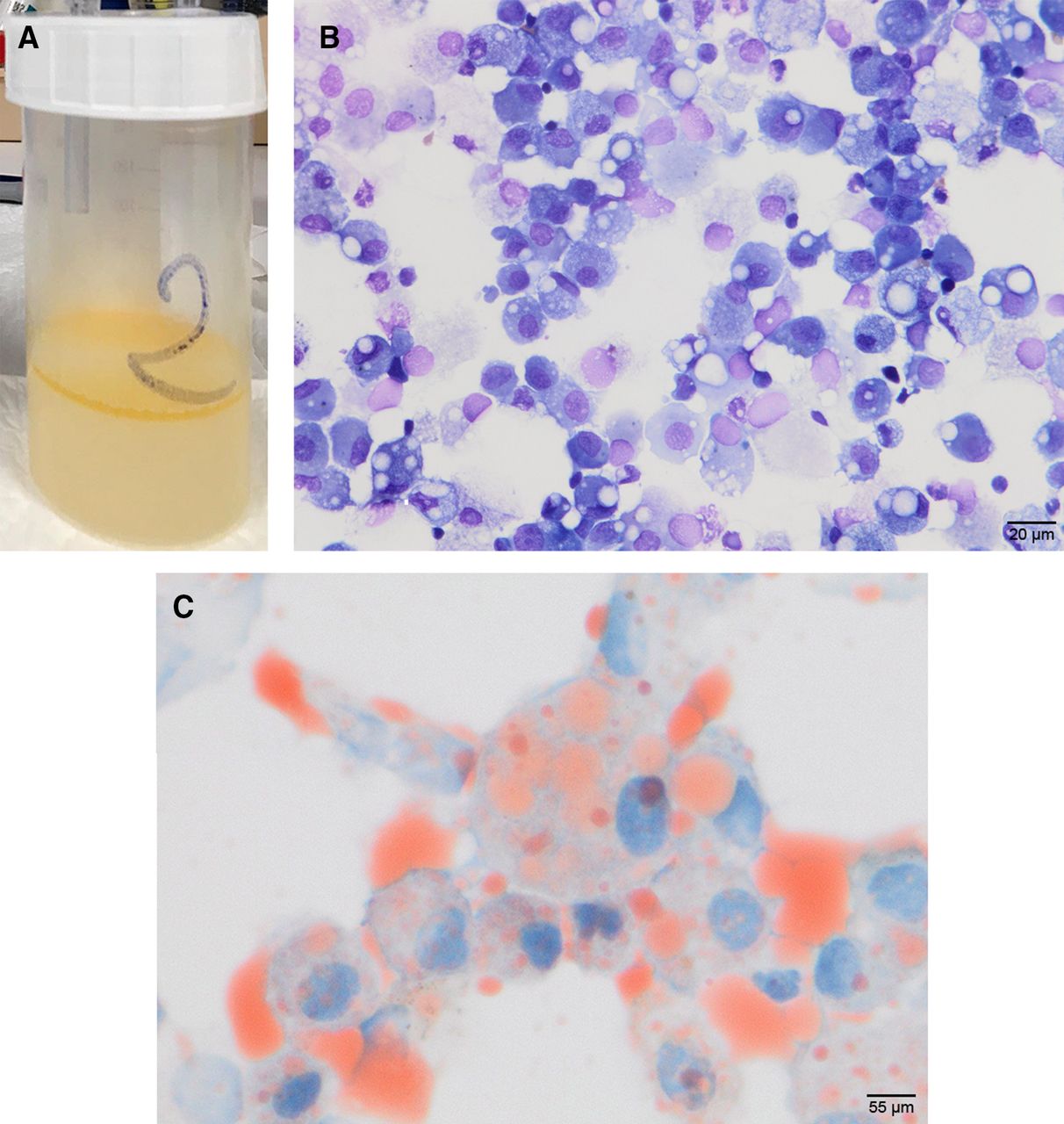
A 51-year-old woman was seen at the emergency department for acute obstructive pyelonephritis diagnosed on an abdominal CT scan that was effectively managed by antibiotics and endoscopic double-J stent. Bilateral ground glass opacities were incidentally observed on the lower parts of the lungs. The patient had recent dyspnoea with normal peripheral oxygen saturation while breathing room air. Lung auscultation revealed bilateral lung crackles. Chest high-resolution CT (HRCT) showed a bilateral ‘crazy-paving pattern’ that, in the context of pandemic was initially considered suggestive of COVID-19 pneumonia, but a nasopharyngeal swab was negative for SARS-CoV-2 by RT-PCR. Strikingly, an air-containing cavity in the anterior mediastinum was also present (figure 1). History revealed that the patient had a prior oesophageal replacement by retrosternal colonic interposition following caustic ingestion 16 years before. A bronchoscopy with bronchoalveolar lavage (BAL) recovered a cream-coloured liquid with a lipid supernatant (figure 2A). BAL cell analysis displayed large optically empty vacuoles within most macrophages (figure 2B), as well as mild (20%) lymphocytic alveolitis. Periodic acid–Schiff staining was negative. Oil red O staining confirmed macrophage lipid accumulation (figure 2C). SARS-CoV-2 RT-PCR in BAL was negative. Bronchial aspiration microscopy revealed acid-fast bacilli identified as Mycobacterium kansasii after culture, considered as colonisation according to the last ATS/ERS/ESCMID/IDSA guidelines.1 The 1-year follow-up showed clinical and radiological improvement without any sign of mycobacterial infection.

High-resolution CT of the chest showing bilateral ground glass opacities with a ‘crazy-paving’ pattern in the lower lobes. Note the presence of an air-containing cavity in the anterior mediastinum corresponding to oesophageal replacement by retrosternal colonic interposition.
{kind=link}
{kind=link}
(A) Cream-coloured liquid with a lipid supernatant recovered by bronchoalveolar lavage. (B) Light microscopy showing alveolar macrophages containing optically empty vacuoles. May-Grunwald-Giemsa staining. original magnification x400. (C) High-power field (×1200) of oil red O colouration demonstrating the lipid content within macrophages.
Resumption of the patient’s interrogation revealed that she consumed dried yoghurt mixed with olive and sunflower oils daily for more than 10 years and had chronic regurgitations responsible for her lipoid pneumonia.
A crazy-paving pattern is a common although non-specific radiological finding characterised by scattered or diffuse ground glass attenuation with superimposed interlobular septal thickening and intralobular lines.2 A large spectrum of lung diseases may exhibit a crazy-paving pattern on HRCT, including infections, classically Pneumocystis jirovecii pneumonia, tumours (lung adenocarcinoma), pulmonary alveolar proteinosis and pulmonary haemorrhage.2 More recently, a crazy-paving pattern has also been reported in a subset of patients with COVID-19 pneumonia.3 Although the distribution of the lung crazy-paving pattern and the presence of additional radiological findings are helpful for discriminating among potential differential diagnoses, lung HRCT alone is not sufficient for a definitive diagnosis.
Exogenous lipoid pneumonia (ELP) is a rare but classical aetiology of lung ground glass opacities that may sometimes appear as a crazy-paving pattern. It is caused by the inhalation or aspiration of mineral, animal or vegetable oil.4 Factors predisposing to aspiration are often identified. Gastrointestinal diseases or surgery that increase the risk of aspiration or regurgitation of gastric contents and neurological diseases are the most common conditions associated with the risk of ELP.5 6 The most common cause of ELP is liquid paraffin used as a laxative and more rarely by fire-eater and oil-based nasal drops.5 6 Recently, ELP has also been reported in several cases of vaping-associated lung injury.7 The exposure to lipid substances may not be obvious at first sight, and repeated history interviews are sometimes required to identify the causative agent. Occasionally, ELP may be complicated by superimposed non-tuberculous mycobacterial colonisation or infection.8
Learning points
Exogenous lipoid pneumonia is a rare but a classical aetiology of crazy-paving pattern on chest CT scan.
A condition favouring oil aspiration or inhalation is present in most cases of exogenous lipoid pneumonia.
Accurate and repeated clinical interview is essential to identify the causative lipid substance.
Ethics statements
Acknowledgments
The authors thank Dr Yaël Amar (Assistance Publique-Hôpitaux de Paris; Service dePneumologie, Hôpital Saint-Louis, Paris, France) for performing the procedure described and providing the bronchoalveolar lavage macroscopic image.
Footnotes
Contributors MC, AB and AT wrote the manuscript. VM reviewed cytological findings and provided the corresponding figures. AB and AT reviewed all chest CT scans and provided the imaging figures. All authors reviewed and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.